S-ar putea să vă placă și
- Dvanced Ardiovascular Ife Upport: A C L SDocument10 paginiDvanced Ardiovascular Ife Upport: A C L SErica Jane100% (1)
- Saudi CPR Guidlines in EnglishDocument16 paginiSaudi CPR Guidlines in EnglishpiyushbamsÎncă nu există evaluări
- Adult Advanced Life SupportDocument23 paginiAdult Advanced Life SupportbigpriapÎncă nu există evaluări
- 23 Mock CodesDocument56 pagini23 Mock Codesmaguisssa100% (4)
- Pediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesDe la EverandPediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesEvaluare: 5 din 5 stele5/5 (2)
- Pediatric Advanced Life Support (PALS) Provider HandbookDe la EverandPediatric Advanced Life Support (PALS) Provider HandbookÎncă nu există evaluări
- Alert Medical Series: Emergency Medicine Alert IIIDe la EverandAlert Medical Series: Emergency Medicine Alert IIIÎncă nu există evaluări
- Prehospital Practice: hypothetically speaking: From classroom to paramedic practice Volume 1 Second editionDe la EverandPrehospital Practice: hypothetically speaking: From classroom to paramedic practice Volume 1 Second editionÎncă nu există evaluări
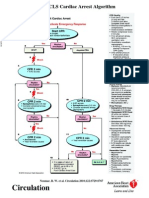
- 2010 Integrated Updated Circulation ACLS Acute Coronary Syndromes AlgorithmDocument1 pagină2010 Integrated Updated Circulation ACLS Acute Coronary Syndromes Algorithmms_lezahÎncă nu există evaluări
- Pals HandoutDocument49 paginiPals HandoutYasir AshfaqÎncă nu există evaluări
- Advanced Paediatric Life Support - A0 PDFDocument1 paginăAdvanced Paediatric Life Support - A0 PDFiulia-uroÎncă nu există evaluări
- ACLS: Advanced Cardiac Life SupportDocument62 paginiACLS: Advanced Cardiac Life SupportAlemayehu beharuÎncă nu există evaluări
- Advanced Life SupportDocument65 paginiAdvanced Life SupportPrasad Narangoda100% (1)
- ACLS and PALS Certification Practice QuestionsDocument11 paginiACLS and PALS Certification Practice Questionsdyah rahayu hutamiÎncă nu există evaluări
- ACLS PRETEST ANSWER KEY RHYTHM IDENTIFICATIONDocument3 paginiACLS PRETEST ANSWER KEY RHYTHM IDENTIFICATIONaditÎncă nu există evaluări
- ToxidromesDocument1 paginăToxidromesMayer Rosenberg100% (7)
- AHA ACLS Written Test: Ready To Study? Start With FlashcardsDocument8 paginiAHA ACLS Written Test: Ready To Study? Start With FlashcardssallyÎncă nu există evaluări
- PALS Precourse Self-AssessmentDocument2 paginiPALS Precourse Self-AssessmentGabriel Del RosarioÎncă nu există evaluări
- APLS Scenario OSCE PDFDocument5 paginiAPLS Scenario OSCE PDFNikita JacobsÎncă nu există evaluări
- ACLS QuizletDocument7 paginiACLS Quizletek.9006001Încă nu există evaluări
- Over View of IAP ALSDocument12 paginiOver View of IAP ALSMohamed RasoolÎncă nu există evaluări
- Pals CardDocument12 paginiPals CardSara KhanÎncă nu există evaluări
- Atls FullDocument82 paginiAtls FullbisturisevenÎncă nu există evaluări
- ACLS Practical Case Scenarios (1 June 2011)Document15 paginiACLS Practical Case Scenarios (1 June 2011)nersÎncă nu există evaluări
- Pepp Als PretestDocument4 paginiPepp Als PretestDave BoppÎncă nu există evaluări
- ACLS Class Packet 2015Document9 paginiACLS Class Packet 2015Chi Wiin100% (3)
- PALS Study GuideDocument12 paginiPALS Study GuidePrerna SehgalÎncă nu există evaluări
- Pediatric Advanced Life Support: I. PALS System Approach AlgorithmDocument19 paginiPediatric Advanced Life Support: I. PALS System Approach AlgorithmIsabel Castillo100% (1)
- Pediatric Mock Resuscitation ScenariosDocument6 paginiPediatric Mock Resuscitation ScenariosdinkytinkÎncă nu există evaluări
- CPR AED Choking Guidelines for Healthcare ProvidersDocument2 paginiCPR AED Choking Guidelines for Healthcare Providersreyes markÎncă nu există evaluări
- Pediatric Cardiac Arrest Algorithm 2020 GuidelinesDocument27 paginiPediatric Cardiac Arrest Algorithm 2020 GuidelinesLinna AndrianiÎncă nu există evaluări
- PALS Algorithms for Shock, Respiratory Emergencies & MoreDocument11 paginiPALS Algorithms for Shock, Respiratory Emergencies & MoreGracia VitaÎncă nu există evaluări
- PICU Common ProblemDocument49 paginiPICU Common ProblemRawabi rawabi1997Încă nu există evaluări
- Advanced Cardiovascular Life Support (ACLS)Document2 paginiAdvanced Cardiovascular Life Support (ACLS)Vijay MgÎncă nu există evaluări
- Adult Basic Life Support Algorithm For Healthcare ProvidersDocument1 paginăAdult Basic Life Support Algorithm For Healthcare ProvidersKavya ShreeÎncă nu există evaluări
- CPR Class QuestionnaireDocument4 paginiCPR Class QuestionnaireParikshit PekhaleÎncă nu există evaluări
- ACLS Algorithms Adult 2010Document12 paginiACLS Algorithms Adult 2010anon_336736395Încă nu există evaluări
- PALS Interim Material 2020 - Provider Manual ChangesDocument3 paginiPALS Interim Material 2020 - Provider Manual ChangesyossyusÎncă nu există evaluări
- ACLS Training - Most Important Points To RememberDocument5 paginiACLS Training - Most Important Points To RememberEman ElzeftawyÎncă nu există evaluări
- Pediatric Advanced Life Support (PALS) - UpToDateDocument49 paginiPediatric Advanced Life Support (PALS) - UpToDateANGIE SIDNEY NARANJO GARCIAÎncă nu există evaluări
- Basic Life Support (BLS) Training Course: FeaturesDocument1 paginăBasic Life Support (BLS) Training Course: FeaturesSheryl Fuentes De GuzmanÎncă nu există evaluări
- Acls Book PDFDocument63 paginiAcls Book PDFSabir Khan67% (3)
- Test 2 OutlineDocument7 paginiTest 2 Outlinemara5140Încă nu există evaluări
- ACLS HandoutsDocument4 paginiACLS HandoutsMeynard AndresÎncă nu există evaluări
- ACLS AlgorithmsDocument4 paginiACLS Algorithmsmonickams100% (1)
- ATLS ProtocolDocument36 paginiATLS ProtocolAmjad AmmarÎncă nu există evaluări
- Basic Ecg 2016Document75 paginiBasic Ecg 2016api-284503860Încă nu există evaluări
- Advanced Trauma Life SupportDocument8 paginiAdvanced Trauma Life SupportAbouzr Mohammed ElsaidÎncă nu există evaluări
- Advanced Trauma Life Support RevisedDocument7 paginiAdvanced Trauma Life Support RevisedpaveethrahÎncă nu există evaluări
- Heartsaver SlidesDocument21 paginiHeartsaver SlidesBelLa EakoiÎncă nu există evaluări
- PALS Provider Manual PDFDocument57 paginiPALS Provider Manual PDFtimie_reyes90% (21)
- 2020 AHA Guidelines For CPR and ECC PrintableDocument21 pagini2020 AHA Guidelines For CPR and ECC PrintableSajal Saha100% (1)
- PALS Pulseless Arrest Algorithm: Kleinman, M. E. Et Al. Circulation 2010 122:S876-S908Document3 paginiPALS Pulseless Arrest Algorithm: Kleinman, M. E. Et Al. Circulation 2010 122:S876-S908YONE LENINÎncă nu există evaluări
- ALS Protocols Complete-RAPID CITY PDFDocument413 paginiALS Protocols Complete-RAPID CITY PDFCh WuÎncă nu există evaluări
- PALS 2015 Update - Nursing Grand RoundsDocument22 paginiPALS 2015 Update - Nursing Grand RoundshatsuneÎncă nu există evaluări
- Introd To ECG Code Blue Champs March 2019Document52 paginiIntrod To ECG Code Blue Champs March 2019james rukenya100% (1)
- ICU Scoring Systems A Complete Guide - 2020 EditionDe la EverandICU Scoring Systems A Complete Guide - 2020 EditionÎncă nu există evaluări
- ACLS Advanced Cardiovascular Life Support Provider Manual 2023De la EverandACLS Advanced Cardiovascular Life Support Provider Manual 2023Încă nu există evaluări
- Microbiology FungusDocument1 paginăMicrobiology Funguszacklim_2000Încă nu există evaluări
- OpthalmologyDocument19 paginiOpthalmologyzacklim_2000Încă nu există evaluări
- Microbiology BacteriaDocument8 paginiMicrobiology Bacteriazacklim_2000Încă nu există evaluări
- Pediatric Chocking AlgoDocument1 paginăPediatric Chocking Algozacklim_2000Încă nu există evaluări
- Newborn Life SupportDocument8 paginiNewborn Life Supportcorn123Încă nu există evaluări
- NlsalgoDocument1 paginăNlsalgozacklim_2000Încă nu există evaluări
- PblsalgoDocument1 paginăPblsalgozacklim_2000Încă nu există evaluări
- Tachycardia AlgorythmDocument1 paginăTachycardia AlgorythmUZNAPMÎncă nu există evaluări
- BlsalgoDocument1 paginăBlsalgozacklim_2000Încă nu există evaluări
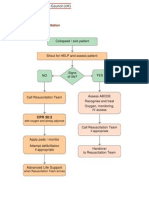
- In Hospital AlgoDocument1 paginăIn Hospital Algozacklim_2000Încă nu există evaluări
- PalsalgoDocument1 paginăPalsalgozacklim_2000Încă nu există evaluări
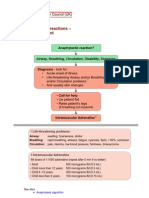
- Resuscitation Council Uk Anaphylaxis AlgorithmDocument1 paginăResuscitation Council Uk Anaphylaxis Algorithmbrianed231100% (1)
- Bra Dal GoDocument1 paginăBra Dal Gozacklim_2000Încă nu există evaluări
- Algorithm Syok AnafilaktikDocument1 paginăAlgorithm Syok AnafilaktikAstriTaufiRamadhaniÎncă nu există evaluări
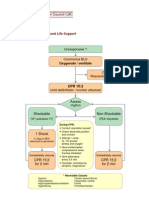
- AlsalgoDocument1 paginăAlsalgozacklim_2000Încă nu există evaluări
- Resuscitation Council (UK)Document18 paginiResuscitation Council (UK)Abdelfattah RashwanÎncă nu există evaluări
- AedalgoDocument1 paginăAedalgozacklim_2000Încă nu există evaluări
- Adult Choking AlgoDocument1 paginăAdult Choking Algozacklim_2000Încă nu există evaluări
- JNC8 & ChlorthalidoneDocument69 paginiJNC8 & ChlorthalidoneAkansha KalraÎncă nu există evaluări
- Metallurgical Failure Analysis of Various ImplantDocument7 paginiMetallurgical Failure Analysis of Various Implantdiegomez84100% (1)
- New LOGIQ e DatasheetDocument10 paginiNew LOGIQ e Datasheetbashir019Încă nu există evaluări
- Final Resume 1Document3 paginiFinal Resume 1api-430931351Încă nu există evaluări
- Chest PhysioDocument6 paginiChest PhysioGoha BashaÎncă nu există evaluări
- What Is A MicrodebriderDocument7 paginiWhat Is A MicrodebriderIqbalurÎncă nu există evaluări
- Principles, Contents, and Steps: Clinical InstructorDocument25 paginiPrinciples, Contents, and Steps: Clinical InstructorWillie KitsÎncă nu există evaluări
- Demata, Andrea Mikaela R. BSN 1E Learning Evidence 2Document6 paginiDemata, Andrea Mikaela R. BSN 1E Learning Evidence 2buttewcupzÎncă nu există evaluări
- 515Document972 pagini515solecitodelmarazul100% (6)
- Damage Control Management in The Polytra PDFDocument462 paginiDamage Control Management in The Polytra PDFFlipÎncă nu există evaluări
- Philippine College of Physicians Daily Census OPD Hospital: (M or F) (S or P)Document2 paginiPhilippine College of Physicians Daily Census OPD Hospital: (M or F) (S or P)filchibuffÎncă nu există evaluări
- Proc PDF FileDocument8 paginiProc PDF FileVivek GutamÎncă nu există evaluări
- Process Recording ExampleDocument7 paginiProcess Recording ExampleCheska ت HortelanoÎncă nu există evaluări
- NeurosurgeonDocument10 paginiNeurosurgeonapi-612131991Încă nu există evaluări
- Avascular Necrosis of The Talus Current Treatment OptionsDocument17 paginiAvascular Necrosis of The Talus Current Treatment Optionssailorgeorge1Încă nu există evaluări
- Amalgam War HistoryDocument10 paginiAmalgam War HistoryDona Randini Ramanayake50% (2)
- IPHS Guidelines Health CentresDocument92 paginiIPHS Guidelines Health CentresdrsanthoshdeepaÎncă nu există evaluări
- Classification of Hearing Loss PDFDocument4 paginiClassification of Hearing Loss PDFAsiya ZaidiÎncă nu există evaluări
- Indian journals indexed in Web of ScienceDocument5 paginiIndian journals indexed in Web of ScienceRAMAKRISHNA VÎncă nu există evaluări
- JaundiceDocument22 paginiJaundiceimanzurynn161Încă nu există evaluări
- Functional OcclusionDocument9 paginiFunctional Occlusionvarsha palledÎncă nu există evaluări
- Panca InderaDocument26 paginiPanca Inderakema_hiperkes100% (1)
- Headache Types and Causes Explained in 40 CharactersDocument16 paginiHeadache Types and Causes Explained in 40 CharactersVenkatesan VidhyaÎncă nu există evaluări
- LaboratoryDocument49 paginiLaboratorybonat0750% (2)
- Lungs 2014Document64 paginiLungs 2014atidÎncă nu există evaluări
- APRN App and Auth To ReleaseDocument5 paginiAPRN App and Auth To ReleaseCourtney SchultÎncă nu există evaluări
- Transient Neonatal Hypocalcemia: Presentation and Outcomes: AuthorsDocument7 paginiTransient Neonatal Hypocalcemia: Presentation and Outcomes: AuthorsMeryÎncă nu există evaluări
- Film ArtifactsDocument43 paginiFilm Artifactskhushi786100% (1)
- IPHS Dist Hosp 201 To 300 Bed StandardsDocument158 paginiIPHS Dist Hosp 201 To 300 Bed StandardsHarshit YadavÎncă nu există evaluări
- NCP Vol 33 No 6 PDFDocument196 paginiNCP Vol 33 No 6 PDFMarwah RifahÎncă nu există evaluări