S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- TM - 1 2840 258 23PDocument276 paginiTM - 1 2840 258 23PSharly_ly80% (5)
- LNG TrainingDocument26 paginiLNG TrainingAnonymous EuI0J1c100% (3)
- Construction Estimate GuideDocument70 paginiConstruction Estimate Guidejanetabunar100% (2)
- Construction Management: Coursera by Columbia UniversityDocument12 paginiConstruction Management: Coursera by Columbia UniversityIggy IgorÎncă nu există evaluări
- Quality ControlDocument7 paginiQuality ControlsamirneseemÎncă nu există evaluări
- Change ManagementDocument35 paginiChange ManagementG_RanjithÎncă nu există evaluări
- Cdc-Guideline For Disinfection and Sterilization in Health-Care Facilities-2008Document158 paginiCdc-Guideline For Disinfection and Sterilization in Health-Care Facilities-2008fuentenatura100% (1)
- Disinfectant Efficacy TestingDocument62 paginiDisinfectant Efficacy TestingG_Ranjith100% (1)
- FDA-Sterility TestDocument14 paginiFDA-Sterility TestG_RanjithÎncă nu există evaluări
- 4230-DS3100 - CompleteBiofilm The Key To Understanding and Controlling Bacterial Growth in Automated Drinking Water SystemsDocument20 pagini4230-DS3100 - CompleteBiofilm The Key To Understanding and Controlling Bacterial Growth in Automated Drinking Water SystemsDr usama El Shafey0% (1)
- Risk AnalysisDocument11 paginiRisk AnalysisG_RanjithÎncă nu există evaluări
- BOD Incubator 2013 RFBDocument7 paginiBOD Incubator 2013 RFBG_RanjithÎncă nu există evaluări
- Non Viable Particle CountDocument14 paginiNon Viable Particle CountG_RanjithÎncă nu există evaluări
- 1320Document20 pagini1320G_RanjithÎncă nu există evaluări
- 0122 09Document6 pagini0122 09G_RanjithÎncă nu există evaluări
- TFF SystemDocument13 paginiTFF SystemG_RanjithÎncă nu există evaluări
- Hemoglobin ConcentrationDocument8 paginiHemoglobin ConcentrationG_RanjithÎncă nu există evaluări
- Risk Management GuidelinesDocument16 paginiRisk Management GuidelinesG_RanjithÎncă nu există evaluări
- 3.2.9. Rubber Closures For Containers For Aqueous Parenteral Preparations, For Powders and For Freeze-Dried PowdersDocument2 pagini3.2.9. Rubber Closures For Containers For Aqueous Parenteral Preparations, For Powders and For Freeze-Dried PowdersG_RanjithÎncă nu există evaluări
- Virology ManualDocument28 paginiVirology ManualG_Ranjith100% (1)
- Aseptic Process ValidationDocument32 paginiAseptic Process ValidationG_Ranjith100% (1)
- 01 2introductionDocument33 pagini01 2introductionG_RanjithÎncă nu există evaluări
- Quality Risk ManagementDocument30 paginiQuality Risk ManagementNenad MihajlovÎncă nu există evaluări
- Toxicology StudiesDocument18 paginiToxicology StudiesG_RanjithÎncă nu există evaluări
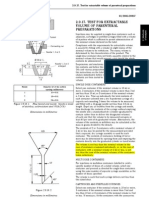
- 2.9.17. Test For Extractable Volume of Parenteral PreparationsDocument2 pagini2.9.17. Test For Extractable Volume of Parenteral PreparationsG_Ranjith100% (4)
- Hands On TFFDocument12 paginiHands On TFFaryan.yaÎncă nu există evaluări
- 6 ParenteralDocument36 pagini6 ParenteralVipin Valappil100% (1)
- 2009 - Le Marché Des AntiveninsDocument45 pagini2009 - Le Marché Des AntiveninsG_RanjithÎncă nu există evaluări
- PassivationDocument7 paginiPassivationG_RanjithÎncă nu există evaluări
- Cleaning Validation StudyDocument12 paginiCleaning Validation StudyG_Ranjith100% (3)
- Future of FMDDocument12 paginiFuture of FMDG_RanjithÎncă nu există evaluări
- SchneiderDocument5 paginiSchneiderG_RanjithÎncă nu există evaluări
- Rounding Off Values in GMPDocument2 paginiRounding Off Values in GMPG_RanjithÎncă nu există evaluări
- DotnetrefDocument130 paginiDotnetrefMárcio BussÎncă nu există evaluări
- DG31PR SpecUpdate07Document6 paginiDG31PR SpecUpdate07usercezarÎncă nu există evaluări
- Ida Aryanie BahrudinDocument44 paginiIda Aryanie BahrudinBDzikri HidayatÎncă nu există evaluări
- About Nordenaudit 2.0Document11 paginiAbout Nordenaudit 2.0Jose DenizÎncă nu există evaluări
- AC 505-005 Issue 01 Aircraft Certification Delegate HandbookDocument46 paginiAC 505-005 Issue 01 Aircraft Certification Delegate Handbookdandylion123Încă nu există evaluări
- Cat-Blaw Knox-VariosDocument156 paginiCat-Blaw Knox-Variosreman parts100% (1)
- Model Estimating: Kevin R. Miller BYU Construction ManagementDocument21 paginiModel Estimating: Kevin R. Miller BYU Construction Managementracing.phreakÎncă nu există evaluări
- PPAPDocument53 paginiPPAPRaajha MunibathiranÎncă nu există evaluări
- Ce12 Moe 2016Document20 paginiCe12 Moe 2016Dawood UllahÎncă nu există evaluări
- Software Testing-1 PDFDocument75 paginiSoftware Testing-1 PDFSai PinakiÎncă nu există evaluări
- Building Insulation BulletinDocument4 paginiBuilding Insulation BulletinSarath ChukkapalliÎncă nu există evaluări
- Harting Conector PDFDocument989 paginiHarting Conector PDFincore1976Încă nu există evaluări
- Catálogo Layher EN - AuV - AluSteg - 600 PDFDocument12 paginiCatálogo Layher EN - AuV - AluSteg - 600 PDFUbiratã AndersonÎncă nu există evaluări
- The Spellman Files by Lisa LutzDocument10 paginiThe Spellman Files by Lisa LutzSimon and SchusterÎncă nu există evaluări
- More Problems in Mechanics Projectile MotionDocument3 paginiMore Problems in Mechanics Projectile MotionBon Axl FeeserÎncă nu există evaluări
- Civil Engineering StandardDocument39 paginiCivil Engineering StandardAli Amzad BhuiyanÎncă nu există evaluări
- PNSMV028Document9 paginiPNSMV028Philippe AlexandreÎncă nu există evaluări
- Hall 08Document1 paginăHall 08chinsy83Încă nu există evaluări
- Validation BootcampDocument281 paginiValidation BootcamplmqasemÎncă nu există evaluări
- Piopoxy AF Tie Coat - TDSDocument2 paginiPiopoxy AF Tie Coat - TDSIsabelo AbaoÎncă nu există evaluări
- Electronic Systems For Modern Construction MachinesDocument15 paginiElectronic Systems For Modern Construction Machinessvinaga100% (1)
- Malaysia Inspection Bodies Accreditation Scheme (Mibas)Document11 paginiMalaysia Inspection Bodies Accreditation Scheme (Mibas)Ko NSÎncă nu există evaluări
- I Holland Tabletting SeminarDocument2 paginiI Holland Tabletting SeminarAKKAD PHARMAÎncă nu există evaluări
- Defects ExclusionDocument12 paginiDefects Exclusionkhurram95103Încă nu există evaluări
- ChecklistDocument28 paginiChecklistphilipalexjonesÎncă nu există evaluări
- Dumping of Printed Circuit BoardDocument2 paginiDumping of Printed Circuit Boardkssanu001Încă nu există evaluări