S-ar putea să vă placă și
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Intmed, ColumnDocument119 paginiIntmed, ColumnLucas AresÎncă nu există evaluări
- ASCIA ADVANCED Acute Management of Anaphylaxis Guidelines 2015Document5 paginiASCIA ADVANCED Acute Management of Anaphylaxis Guidelines 2015Lucas AresÎncă nu există evaluări
- Acute Pumonary EdemaDocument7 paginiAcute Pumonary EdemaLucas AresÎncă nu există evaluări
- Acute Pumonary EdemaDocument6 paginiAcute Pumonary EdemaLucas AresÎncă nu există evaluări
- 6.-Metabolism Obesity DM PDFDocument98 pagini6.-Metabolism Obesity DM PDFLucasÎncă nu există evaluări
- ASCIA Guidelines Acute Management Anaphylaxis Dec2016Document5 paginiASCIA Guidelines Acute Management Anaphylaxis Dec2016kkkssbbÎncă nu există evaluări
- GPC 466 Ictus AP Lain Entr Compl enDocument230 paginiGPC 466 Ictus AP Lain Entr Compl enLucas AresÎncă nu există evaluări
- Analgesia & Sedaton in PICUDocument5 paginiAnalgesia & Sedaton in PICULucas AresÎncă nu există evaluări
- GPC 466 Ictus AP Lain Entr Compl enDocument230 paginiGPC 466 Ictus AP Lain Entr Compl enLucas AresÎncă nu există evaluări
- 2 Biliary PancreasDocument87 pagini2 Biliary PancreasLucas AresÎncă nu există evaluări
- Pathology of Injury, Cell Death and InjuryDocument88 paginiPathology of Injury, Cell Death and InjuryLucas AresÎncă nu există evaluări
- Congenital and Neonatal InfectionsDocument9 paginiCongenital and Neonatal InfectionsLucas AresÎncă nu există evaluări
- 1 Path of The LiverDocument97 pagini1 Path of The LiverLucas AresÎncă nu există evaluări
- Congenital and Neonatal InfectionsDocument108 paginiCongenital and Neonatal InfectionsMinerva StanciuÎncă nu există evaluări
- Acute Pumonary EdemaDocument7 paginiAcute Pumonary EdemaLucas AresÎncă nu există evaluări
- Classification of Interferons (Ifns) : Interferons and Chemokines Cytokine Receptors/Signaling Adhesion MoleculesDocument10 paginiClassification of Interferons (Ifns) : Interferons and Chemokines Cytokine Receptors/Signaling Adhesion MoleculesLucas AresÎncă nu există evaluări
- 5 - The Propagation of The Action Potential in Nerve FibersDocument2 pagini5 - The Propagation of The Action Potential in Nerve FibersLucas AresÎncă nu există evaluări
- 2 - Membrane Transport MechanismsDocument2 pagini2 - Membrane Transport MechanismsLucas AresÎncă nu există evaluări
- 6 - Electrotonic PotentialsDocument1 pagină6 - Electrotonic PotentialsLucas AresÎncă nu există evaluări
- 3 - The Resting Membrane PotentialDocument1 pagină3 - The Resting Membrane PotentialLucas AresÎncă nu există evaluări
- 4 - The Action Potential in Nerve FibersDocument2 pagini4 - The Action Potential in Nerve FibersLucas AresÎncă nu există evaluări
- 1 - General Principles of Control TheoryDocument2 pagini1 - General Principles of Control TheoryLucas AresÎncă nu există evaluări
- 1 - Cellular Injury Calcification Pathology PresentationDocument91 pagini1 - Cellular Injury Calcification Pathology PresentationLucas AresÎncă nu există evaluări
- Antigens, Microbiology PresentationDocument8 paginiAntigens, Microbiology PresentationLucas AresÎncă nu există evaluări
- Drugs AdministrationDocument37 paginiDrugs AdministrationLucas AresÎncă nu există evaluări
- Basic Invasive ProceduresDocument39 paginiBasic Invasive ProceduresLucas AresÎncă nu există evaluări
- 2014 3 06 Cortex Cerebri enDocument58 pagini2014 3 06 Cortex Cerebri enLucas AresÎncă nu există evaluări
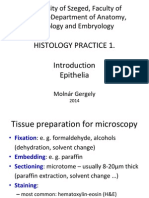
- 2 01 Epithelia 2014Document47 pagini2 01 Epithelia 2014Lucas AresÎncă nu există evaluări
- 2014 3 05 Nuclei BasalesDocument66 pagini2014 3 05 Nuclei BasalesLucas AresÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (120)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Diet Pra Pasca BedahDocument22 paginiDiet Pra Pasca BedahMuhammad AÎncă nu există evaluări
- UC Davis Koret Shelter Medicine Program - Feline Leukemia Virus (FeLV) - 2012-04-25Document3 paginiUC Davis Koret Shelter Medicine Program - Feline Leukemia Virus (FeLV) - 2012-04-25Kitt KaosÎncă nu există evaluări
- 54750174Document3 pagini54750174Rouwi DesiatcoÎncă nu există evaluări
- Makassed Experience in Management of Placenta AccretaDocument39 paginiMakassed Experience in Management of Placenta AccretaRaluca HabaÎncă nu există evaluări
- Daftar Pustaka PDFDocument3 paginiDaftar Pustaka PDFRatih Ayu PÎncă nu există evaluări
- Hypertension BrochureDocument2 paginiHypertension BrochureDenzelita BelgraveÎncă nu există evaluări
- Role of LABACS Provides A Simple and Effective For COPD and Asthma ManagementDocument74 paginiRole of LABACS Provides A Simple and Effective For COPD and Asthma ManagementHans WinardiÎncă nu există evaluări
- MSN Ii - 24.6.2020 An-Tonsillitis and AdenoiditisDocument41 paginiMSN Ii - 24.6.2020 An-Tonsillitis and AdenoiditisYAMINIPRIYANÎncă nu există evaluări
- Case Study of Acute GastritisDocument12 paginiCase Study of Acute Gastritisstudent_01960% (5)
- Pep 2021 - October QuestionsDocument4 paginiPep 2021 - October QuestionsCynthia ObiÎncă nu există evaluări
- Acute Medicine (Medical Masterclass)Document163 paginiAcute Medicine (Medical Masterclass)Chris Jardine Li100% (1)
- Lesson Plan: S.No Objectives Content Method of Teaching/ Teaching Aid Time in Min EvaluationDocument2 paginiLesson Plan: S.No Objectives Content Method of Teaching/ Teaching Aid Time in Min EvaluationNaqash HamayunÎncă nu există evaluări
- Quiz7 Follow-Up MCQS: (Answers Below!) MCQ: @urologyquizDocument2 paginiQuiz7 Follow-Up MCQS: (Answers Below!) MCQ: @urologyquizUrologyQuizÎncă nu există evaluări
- Nursing Care Plan For: Diabetes, High Blood Sugar, Hyperglycemia, DKA, Diabetic Ketoacidosis, Fluid and Electrolytes ImbalanceDocument2 paginiNursing Care Plan For: Diabetes, High Blood Sugar, Hyperglycemia, DKA, Diabetic Ketoacidosis, Fluid and Electrolytes ImbalanceFhai EscioÎncă nu există evaluări
- Risk Assessment Envirn Mad Cow Disease-2Document9 paginiRisk Assessment Envirn Mad Cow Disease-2api-436969344Încă nu există evaluări
- NURSING CARE PLAN 2 - Written ReportDocument3 paginiNURSING CARE PLAN 2 - Written ReportAkira PinedaÎncă nu există evaluări
- HemorrhoidsDocument26 paginiHemorrhoidsWaqar ZahirÎncă nu există evaluări
- Spinal Tumors Intra-Extra (Turgut Tali)Document92 paginiSpinal Tumors Intra-Extra (Turgut Tali)Drbaddireddy RayuduÎncă nu există evaluări
- Breast CancerDocument129 paginiBreast CancerHope LeeÎncă nu există evaluări
- Introduction To Clinical Neurology: Acute Low Back and Neck PainDocument64 paginiIntroduction To Clinical Neurology: Acute Low Back and Neck PainKhan A RehÎncă nu există evaluări
- EKG Rhythms2 PDFDocument7 paginiEKG Rhythms2 PDFAya KamajayaÎncă nu există evaluări
- Chapter One 1.1 Background of The StudyDocument46 paginiChapter One 1.1 Background of The StudyUsman Ahmad Tijjani100% (1)
- BioFire BrochureDocument3 paginiBioFire BrochureETÎncă nu există evaluări
- Transcription WHO MOOC AMR ModuleI ENDocument6 paginiTranscription WHO MOOC AMR ModuleI ENANGELO FERRÃOÎncă nu există evaluări
- Case 3.1Document11 paginiCase 3.1atdumagÎncă nu există evaluări
- Abdominal Paracentesis.Document4 paginiAbdominal Paracentesis.Sukh Preet100% (1)
- Cause and Effect EssayDocument10 paginiCause and Effect EssayМолдабекова АйсулуÎncă nu există evaluări
- Anestesi Text Book ReadingDocument5 paginiAnestesi Text Book Readingli2delÎncă nu există evaluări
- AXR Made EasyDocument13 paginiAXR Made EasycswathikanÎncă nu există evaluări
- (Stasi) How To Approach Thrombocytopenia PDFDocument7 pagini(Stasi) How To Approach Thrombocytopenia PDFrodtobingÎncă nu există evaluări