S-ar putea să vă placă și
- Interpreting Product LabelsDocument16 paginiInterpreting Product LabelsHarlynCalimpongLarano100% (1)
- Final DLCDocument28 paginiFinal DLCHardy MisagalÎncă nu există evaluări
- Welcome to Grade Six MixturesDocument24 paginiWelcome to Grade Six MixturesRIALIZA TRANGIAÎncă nu există evaluări
- Grade 6 PE Quarter 1 Lesson 2 ComponentsDocument38 paginiGrade 6 PE Quarter 1 Lesson 2 ComponentsRaymund QuisiquisiÎncă nu există evaluări
- DLL - Science 6 - Q2 - W1Document10 paginiDLL - Science 6 - Q2 - W1Erika ShoppeeÎncă nu există evaluări
- LAMP Arts 2Document5 paginiLAMP Arts 2Lorenz Chiong CariagaÎncă nu există evaluări
- Ashlee Mammenga Two Prong Lesson Plan 1Document3 paginiAshlee Mammenga Two Prong Lesson Plan 1api-252244536Încă nu există evaluări
- DLP in Mathematics 4 Quarter 4Document11 paginiDLP in Mathematics 4 Quarter 4Lorina GallegoÎncă nu există evaluări
- Answer SheetDocument4 paginiAnswer Sheetmae santosÎncă nu există evaluări
- DLL - Mapeh 6 - Q3 - W4Document4 paginiDLL - Mapeh 6 - Q3 - W4Lesli Daryl Antolin SanMateo100% (1)
- Mapeh - P.E. 6: First Quarter-Module 1Document9 paginiMapeh - P.E. 6: First Quarter-Module 1NICOLE ALANAÎncă nu există evaluări
- DLL English Aug 29-Sept 2Document2 paginiDLL English Aug 29-Sept 2IvanAbandoÎncă nu există evaluări
- Budget of Work in Music, Arts, Physical Education, Health (Mapeh) 2Document5 paginiBudget of Work in Music, Arts, Physical Education, Health (Mapeh) 2KeyrenÎncă nu există evaluări
- Grade 3 DLL MAPEH 3 Q1 Week 3Document5 paginiGrade 3 DLL MAPEH 3 Q1 Week 3Jahyala KristalÎncă nu există evaluări
- Describes The Nature and Background of 2. Undertakes Physical Activity and PhysicalDocument2 paginiDescribes The Nature and Background of 2. Undertakes Physical Activity and PhysicalSerLem WellÎncă nu există evaluări
- MASILE ELEMENTARY SCHOOL FIRST PERIODICAL TEST IN SCIENCEDocument5 paginiMASILE ELEMENTARY SCHOOL FIRST PERIODICAL TEST IN SCIENCEAhmie Javier CabantogÎncă nu există evaluări
- English Lesson Exemplar Cot 2Document3 paginiEnglish Lesson Exemplar Cot 2Fred Ryan Canoy DeañoÎncă nu există evaluări
- Elementary school lesson plan on number sequences and patternsDocument2 paginiElementary school lesson plan on number sequences and patternsFrancia Yalung Jimenez Galang100% (1)
- DLL - English 3 - Q1 - W1Document3 paginiDLL - English 3 - Q1 - W1Rachael Sales DifuntorumÎncă nu există evaluări
- DLL - Science 6 - Q2 - W6Document10 paginiDLL - Science 6 - Q2 - W6Geoffrey Tolentino-UnidaÎncă nu există evaluări
- MAPEH Budget of Work for Grade 1 in Davao del NorteDocument46 paginiMAPEH Budget of Work for Grade 1 in Davao del NorteMigs Migs MigsÎncă nu există evaluări
- Detailed Lesson Plan in English ThreeDocument4 paginiDetailed Lesson Plan in English ThreeGem DayaoÎncă nu există evaluări
- Explicit Lesson Plan in MTB3-COT1Document4 paginiExplicit Lesson Plan in MTB3-COT1Helen A. Bustamante100% (1)
- EPP-Agriculture 6 3 Week 2: Learning Area Grade Level Quarter DateDocument4 paginiEPP-Agriculture 6 3 Week 2: Learning Area Grade Level Quarter DateJari CruzÎncă nu există evaluări
- Lesson Plan in HealthDocument7 paginiLesson Plan in HealthAcess EmanezÎncă nu există evaluări
- DLL - Science 3 - Q1 - W7Document3 paginiDLL - Science 3 - Q1 - W7Pergie Acabo TelarmaÎncă nu există evaluări
- Midterm Pe104 21920Document3 paginiMidterm Pe104 21920navie VÎncă nu există evaluări
- The Magical Sounds and Symbolic Movements of the Maglalatik DanceDocument3 paginiThe Magical Sounds and Symbolic Movements of the Maglalatik DanceMelchor LumayagÎncă nu există evaluări
- Exploring Useful and Harmful Materials in Science (Grade 5)Document5 paginiExploring Useful and Harmful Materials in Science (Grade 5)timothy castilloÎncă nu există evaluări
- 3.4. Simple Folk Dance StepsDocument3 pagini3.4. Simple Folk Dance StepsMa Josielyn QuimingÎncă nu există evaluări
- Music Melcs Grade 1Document3 paginiMusic Melcs Grade 1Vincent Pol AsioÎncă nu există evaluări
- 4 Science Light Sound Quiz RubricDocument1 pagină4 Science Light Sound Quiz Rubricapi-282532318Încă nu există evaluări
- Prevention of Substance Use and Abuse (Gateway Drugs: Cigarette and AlcoholDocument11 paginiPrevention of Substance Use and Abuse (Gateway Drugs: Cigarette and AlcoholYuki雪Încă nu există evaluări
- Detailed Lesson Plan (Mixture Characteristics)Document8 paginiDetailed Lesson Plan (Mixture Characteristics)Kevin De GuzmanÎncă nu există evaluări
- Calculations in analytical chemistryDocument17 paginiCalculations in analytical chemistryXyza Frea TaizaÎncă nu există evaluări
- Eng 4 q1 Wk6 Day 2Document9 paginiEng 4 q1 Wk6 Day 2maribeth amor-sananoÎncă nu există evaluări
- Regional Training on Critical Content in Grade 8 ScienceDocument6 paginiRegional Training on Critical Content in Grade 8 ScienceFe GullodÎncă nu există evaluări
- Master's curriculum theory course syllabusDocument3 paginiMaster's curriculum theory course syllabusFloorÎncă nu există evaluări
- Describe What Happens When Solids Are Mixed WithDocument7 paginiDescribe What Happens When Solids Are Mixed WithSong Soo JaeÎncă nu există evaluări
- Maintaining Healthy HabitsDocument3 paginiMaintaining Healthy HabitsumikaÎncă nu există evaluări
- Kunday Kumintang Kunday Kumintang Kunday Kunday-Kunday KumintangDocument3 paginiKunday Kumintang Kunday Kumintang Kunday Kunday-Kunday KumintangApril Catadman QuitonÎncă nu există evaluări
- Mapeh - P.E. 6: First Quarter-Module 3 Topic: Skills Involved in Playing GamesDocument8 paginiMapeh - P.E. 6: First Quarter-Module 3 Topic: Skills Involved in Playing GamesNICOLE ALANA100% (1)
- Least Learned CompetencyDocument2 paginiLeast Learned Competencygladys baldeoÎncă nu există evaluări
- English 5Document25 paginiEnglish 5Menchie Salvana BaringÎncă nu există evaluări
- Budget of Work Science 6Document3 paginiBudget of Work Science 6G6 MapagmahalÎncă nu există evaluări
- Least Learned MAPEH Competencies Obillo ElementaryDocument4 paginiLeast Learned MAPEH Competencies Obillo ElementaryRaulJunioRamos100% (1)
- Detailed Lesson Plan in Science VI (GRavity)Document7 paginiDetailed Lesson Plan in Science VI (GRavity)Azia GoniloamusÎncă nu există evaluări
- LAC Session Program For ScienceDocument1 paginăLAC Session Program For ScienceJessica Curay Salugsugan100% (1)
- Elementary Science Lesson on MixturesDocument9 paginiElementary Science Lesson on MixturesIvanAbando100% (1)
- Physical Education K-12 EssentialsDocument47 paginiPhysical Education K-12 EssentialsEmerald ReyesÎncă nu există evaluări
- Math Lesson Logs for Grades 1-12Document5 paginiMath Lesson Logs for Grades 1-12Pauline Erika CagampangÎncă nu există evaluări
- Table of Specification First Quarter - English 2: EN2PA-Ia-c-1.1 En2Bpk - Ib-C-4 EN2G-Ib - c-1.4 En2Ol - I h-j-1.3.2Document2 paginiTable of Specification First Quarter - English 2: EN2PA-Ia-c-1.1 En2Bpk - Ib-C-4 EN2G-Ib - c-1.4 En2Ol - I h-j-1.3.2JENNIFER MAGPANTAYÎncă nu există evaluări
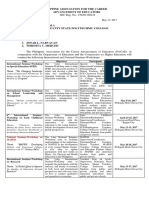
- Philippine Educators Seminar Workshops 2017Document2 paginiPhilippine Educators Seminar Workshops 2017NaruffRalliburÎncă nu există evaluări
- DLL in MAPEH 6, July 2-6, 2018Document4 paginiDLL in MAPEH 6, July 2-6, 2018Malmon TabetsÎncă nu există evaluări
- DAILY LESSON Plan Lesson 24Document2 paginiDAILY LESSON Plan Lesson 24Robert JamesÎncă nu există evaluări
- Englishh WK8 - L 35Document26 paginiEnglishh WK8 - L 35Rowena CaluyaÎncă nu există evaluări
- (DCLM Iii.A1) : DCLM III. Local Beliefs and Values (DCLM III.A1) Paghigugma, Pangulitawo, PangasawaDocument18 pagini(DCLM Iii.A1) : DCLM III. Local Beliefs and Values (DCLM III.A1) Paghigugma, Pangulitawo, PangasawaLeachez Bbdear BarbaÎncă nu există evaluări
- Activity Sheet In: Mapeh (Music)Document12 paginiActivity Sheet In: Mapeh (Music)Rox EstandaÎncă nu există evaluări
- Understanding Personal Health IssuesDocument5 paginiUnderstanding Personal Health IssuesCathlyn Joy GanadenÎncă nu există evaluări
- Monthly Accomplishment Report District OfficeDocument2 paginiMonthly Accomplishment Report District OfficeMaria Victoria Malonzo AcostaÎncă nu există evaluări
- BlankSHN Form 021 District Nutritional Status ReportDocument1 paginăBlankSHN Form 021 District Nutritional Status ReportMaria Victoria Malonzo AcostaÎncă nu există evaluări
- Request Form137Document1 paginăRequest Form137Maria Victoria Malonzo AcostaÎncă nu există evaluări
- 2019jul22rhia1111pds2018PDS - REVISEDDocument14 pagini2019jul22rhia1111pds2018PDS - REVISEDMaria Victoria Malonzo AcostaÎncă nu există evaluări
- Criiria. CHIFdocxDocument1 paginăCriiria. CHIFdocxMaria Victoria Malonzo AcostaÎncă nu există evaluări
- Improve Reading Fluency with Repeated ReadingDocument7 paginiImprove Reading Fluency with Repeated ReadingMaria Victoria Malonzo AcostaÎncă nu există evaluări
- The Analytic Method of Teaching - RyanDocument25 paginiThe Analytic Method of Teaching - RyanMaria Victoria Malonzo AcostaÎncă nu există evaluări
- RPFT PresentationDocument46 paginiRPFT PresentationSusan Valerio ElladoÎncă nu există evaluări
- Classification, Pathophysiology, Diagnosis and Management of DiabetesDocument19 paginiClassification, Pathophysiology, Diagnosis and Management of DiabeteswakhidrizkaÎncă nu există evaluări
- Adolescents, Young Adults and AdultsDocument13 paginiAdolescents, Young Adults and AdultsTharhata JuhasanÎncă nu există evaluări
- Arterijska Hipertenzija U Osoba Starije Životne DobiDocument5 paginiArterijska Hipertenzija U Osoba Starije Životne DobiRebecca BlackburnÎncă nu există evaluări
- Kuesioner GHQ 12Document11 paginiKuesioner GHQ 12Maria Magdalena Lumban GaolÎncă nu există evaluări
- Pharmaceutical: PhilippinesDocument29 paginiPharmaceutical: PhilippinesHealthEconomicsÎncă nu există evaluări
- College of Nursing and Allied Medical Sciences: WesleyanDocument5 paginiCollege of Nursing and Allied Medical Sciences: WesleyanPrince Juzzel BanagÎncă nu există evaluări
- Chem Project HiteshDocument16 paginiChem Project HiteshSahil Sharma64% (14)
- Effectiveness of structured teaching programme on knowledge regarding effect of junk foodDocument156 paginiEffectiveness of structured teaching programme on knowledge regarding effect of junk foodCynthia Joy IbhafidonÎncă nu există evaluări
- Identifying Nutrients in FoodDocument4 paginiIdentifying Nutrients in Foodapi-263340585Încă nu există evaluări
- Routine Diary - EditableDocument3 paginiRoutine Diary - EditableSarah GrundyÎncă nu există evaluări
- Service Management at Gold's GymDocument12 paginiService Management at Gold's GymSushant Suryakant NadargeÎncă nu există evaluări
- Pe10 TG U2Document81 paginiPe10 TG U2lorraine uy50% (4)
- Swimming TechniqueDocument32 paginiSwimming TechniqueTrainer Aong80% (5)
- CEDA-2023-Programme Final Pentru SiteDocument24 paginiCEDA-2023-Programme Final Pentru SiteMaricela IvașcuÎncă nu există evaluări
- Shea ButterDocument133 paginiShea Buttererica2012Încă nu există evaluări
- Pituitary DisordersDocument65 paginiPituitary Disordersgema disiyuna100% (1)
- Healthmedicinet Com II 2014 MayDocument381 paginiHealthmedicinet Com II 2014 MayHeal ThmedicinetÎncă nu există evaluări
- Prevalence, Knowledge and Preventive Practices Against Hypertension Among Police Officers in IbadanDocument8 paginiPrevalence, Knowledge and Preventive Practices Against Hypertension Among Police Officers in Ibadaninna mayaÎncă nu există evaluări
- Angina Symptoms, Causes, Tests and TreatmentDocument33 paginiAngina Symptoms, Causes, Tests and TreatmentAnonymous mIw67bMXÎncă nu există evaluări
- Tr90 Flyer Eng (4 Pages)Document4 paginiTr90 Flyer Eng (4 Pages)Cherry San DiegoÎncă nu există evaluări
- ING 112A Final Exam Practice - OBESITYDocument3 paginiING 112A Final Exam Practice - OBESITYokyayisil0735Încă nu există evaluări
- History - CushingDocument6 paginiHistory - CushingNur FadzreenaÎncă nu există evaluări
- The Body Rescue BookDocument95 paginiThe Body Rescue BookagaÎncă nu există evaluări
- Literature Review Tabitha Satkamp 2Document4 paginiLiterature Review Tabitha Satkamp 2api-608392349Încă nu există evaluări
- Dr. Daniel H. Bessesen: The Biology of ObesityDocument58 paginiDr. Daniel H. Bessesen: The Biology of ObesityNational Press FoundationÎncă nu există evaluări
- The Impact On Metabolic and Reproductive Diseases of Low-Carbohydrate and Ketogenic DietsDocument10 paginiThe Impact On Metabolic and Reproductive Diseases of Low-Carbohydrate and Ketogenic DietsRonell Ernesto GonzalezÎncă nu există evaluări
- Midterm Trans 2 - Metabolic and Bariatric Surgery PDFDocument4 paginiMidterm Trans 2 - Metabolic and Bariatric Surgery PDFErneslito LucasÎncă nu există evaluări
- Young Fatal Case of Familial Hypercholesterolemia: A Case ReportDocument2 paginiYoung Fatal Case of Familial Hypercholesterolemia: A Case ReportPeertechz Publications Inc.Încă nu există evaluări
- Black Iron Beast - 5 - 3 - 1 CalculatorDocument9 paginiBlack Iron Beast - 5 - 3 - 1 CalculatorGiovanni FortÎncă nu există evaluări