S-ar putea să vă placă și
- Interpreting PDX Dot BlotsDocument2 paginiInterpreting PDX Dot BlotsSpy CameraÎncă nu există evaluări
- Managing Renal FailureDocument10 paginiManaging Renal Failuretaner_soysurenÎncă nu există evaluări
- 2022 - Call For Applications-Maine - GRADDocument1 pagină2022 - Call For Applications-Maine - GRADCárdenas EfrainÎncă nu există evaluări
- Retrovirus Educational Toolkit: Sponsored byDocument16 paginiRetrovirus Educational Toolkit: Sponsored byCárdenas EfrainÎncă nu există evaluări
- Feline Herpesvirus Infection: VirusDocument25 paginiFeline Herpesvirus Infection: VirusCárdenas EfrainÎncă nu există evaluări
- ProP Splenectomy Hilar Ligation TechniqueDocument7 paginiProP Splenectomy Hilar Ligation TechniqueCárdenas EfrainÎncă nu există evaluări
- Climate Change and Marine Turtles: ReviewDocument18 paginiClimate Change and Marine Turtles: ReviewThe Science Exchange International Sea Turtle InternshipsÎncă nu există evaluări
- Ecología de Enfermedades EmergentesDocument14 paginiEcología de Enfermedades EmergentesCárdenas EfrainÎncă nu există evaluări
- Paper 2Document5 paginiPaper 2Cárdenas EfrainÎncă nu există evaluări
- Paper 2 PDFDocument5 paginiPaper 2 PDFCárdenas EfrainÎncă nu există evaluări
- Toxicology and Applied Pharmacology: Kevin R. Smith, David Leonard, Jacob D. Mcdonald, Yohannes TesfaigziDocument8 paginiToxicology and Applied Pharmacology: Kevin R. Smith, David Leonard, Jacob D. Mcdonald, Yohannes TesfaigziCárdenas EfrainÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Ozone - A Wide Spectrum Healer by Gary Null PHDDocument20 paginiOzone - A Wide Spectrum Healer by Gary Null PHDangelakimba100% (4)
- Atrya BroucherDocument5 paginiAtrya BroucherAkash SelokarÎncă nu există evaluări
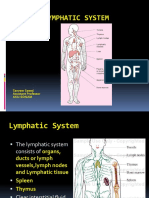
- Lymphatic System Part 1Document33 paginiLymphatic System Part 1NaveelaÎncă nu există evaluări
- Medicinal Mushrooms C HobbsDocument38 paginiMedicinal Mushrooms C HobbsAnatole33100% (7)
- FOUNDATION OF CONTROL QUESTIONS OF EXAM 2020-2021 General MedicineDocument7 paginiFOUNDATION OF CONTROL QUESTIONS OF EXAM 2020-2021 General MedicineSoz P. KawaniÎncă nu există evaluări
- Imunodeficituri Daavadebebi: Manana ToduaDocument21 paginiImunodeficituri Daavadebebi: Manana ToduaManana IsayevaÎncă nu există evaluări
- SOFW Dec2010Document80 paginiSOFW Dec2010kmsrajuÎncă nu există evaluări
- Techniques For Immune Function Analysis HandbookDocument248 paginiTechniques For Immune Function Analysis HandbookDante AvilésÎncă nu există evaluări
- EndosulfanDocument41 paginiEndosulfanbelkira69Încă nu există evaluări
- NeoplasiaDocument150 paginiNeoplasiaDavon Richard Walter Van-VeenÎncă nu există evaluări
- 2-1 Introduction: 2-2 The Atomic Origin of MagnetismDocument30 pagini2-1 Introduction: 2-2 The Atomic Origin of Magnetismجابر الطوكيÎncă nu există evaluări
- General Anatomy of The Immune SystemDocument29 paginiGeneral Anatomy of The Immune Systemrambabs369100% (2)
- Yang 2017Document10 paginiYang 2017wendyÎncă nu există evaluări
- Prebiotics, Probiotics and SynbioticsDocument42 paginiPrebiotics, Probiotics and SynbioticsDrKrishna DasÎncă nu există evaluări
- Immuno-Histochemistry: Alexander E. KalyuzhnyDocument91 paginiImmuno-Histochemistry: Alexander E. KalyuzhnyAlfianti Rahma NingtyasÎncă nu există evaluări
- Varela Etal 2022 Lycopene in MalariaDocument31 paginiVarela Etal 2022 Lycopene in MalariaNathália AraújoÎncă nu există evaluări
- Immuno SeroDocument80 paginiImmuno SeroDocAxi Maximo Jr AxibalÎncă nu există evaluări
- Inflammation and Inflammatory MediatorsDocument40 paginiInflammation and Inflammatory MediatorsQuty Papa KannaÎncă nu există evaluări
- Syllabus For 5-Years Integrated M. Sc. Degree: UM-DAE Centre For Excellence in Basic SciencesDocument92 paginiSyllabus For 5-Years Integrated M. Sc. Degree: UM-DAE Centre For Excellence in Basic SciencesAubal ShaubalÎncă nu există evaluări
- Monoclonal Antibody: Engineering and TherapyDocument39 paginiMonoclonal Antibody: Engineering and TherapyAugusta Rizki AnandaÎncă nu există evaluări
- Government Laws and Policies About Hiv and Aids: Presented By: Group 4Document11 paginiGovernment Laws and Policies About Hiv and Aids: Presented By: Group 4Jerico HensonÎncă nu există evaluări
- Vaccine - WikipediaDocument31 paginiVaccine - WikipediaJohnÎncă nu există evaluări
- HIV AIDS NCLEX Questions Nursing Review QuizDocument10 paginiHIV AIDS NCLEX Questions Nursing Review QuizShella Mae UsquisaÎncă nu există evaluări
- Breastfeeding More Than Just Good Nutrition PDFDocument19 paginiBreastfeeding More Than Just Good Nutrition PDFAndini Pramono100% (1)
- Atopic Disease Bronchial AsthmaDocument33 paginiAtopic Disease Bronchial AsthmaEmeraldyModyÎncă nu există evaluări
- Generalov-II - Medical Microbiology Virology Immunology - Pt-1 - 2016 PDFDocument282 paginiGeneralov-II - Medical Microbiology Virology Immunology - Pt-1 - 2016 PDFgmdÎncă nu există evaluări
- 1284971977vitamin Supp NeofarmaDocument9 pagini1284971977vitamin Supp NeofarmaRaza Un NabiÎncă nu există evaluări
- Lypm Immunity SystemDocument22 paginiLypm Immunity SystemPhoenix JudgeÎncă nu există evaluări
- Biological Theory 1Document28 paginiBiological Theory 1jhonnyscottÎncă nu există evaluări
- The Biology of Evil - Part 2Document65 paginiThe Biology of Evil - Part 2Gavin Soccorso100% (1)