S-ar putea să vă placă și
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- 2 Step Dermoscopedia SmallDocument4 pagini2 Step Dermoscopedia SmallAndreea Barbuta100% (2)
- Cancer Risk Evaluation in PsoriasisDocument3 paginiCancer Risk Evaluation in PsoriasisAndreea BarbutaÎncă nu există evaluări
- 20.pielea Si Derivatele EiDocument9 pagini20.pielea Si Derivatele EiAndreea BarbutaÎncă nu există evaluări
- Jid 2009113 ADocument9 paginiJid 2009113 AAMELIA.SYAHUTAMIÎncă nu există evaluări
- Weekly To Dos PDFDocument1 paginăWeekly To Dos PDFNovia Rizki AmaliaÎncă nu există evaluări
- Monthly Planner November PDFDocument1 paginăMonthly Planner November PDFJethro LemosneroÎncă nu există evaluări
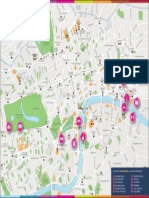
- London Tourist MapDocument1 paginăLondon Tourist MapAmber RileyÎncă nu există evaluări
- Sep. 2013 CollectionDocument14 paginiSep. 2013 CollectionAndreea BarbutaÎncă nu există evaluări
- Tuesday, January 11, 2011Document1 paginăTuesday, January 11, 2011Andreea BarbutaÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- RBH AxiomV Catalog v2011Document16 paginiRBH AxiomV Catalog v2011Sundar RamasamyÎncă nu există evaluări
- Technical Analysis 1: Lg/Med Track ExcavatorsDocument6 paginiTechnical Analysis 1: Lg/Med Track ExcavatorsKang AdingÎncă nu există evaluări
- API TutorialDocument22 paginiAPI TutorialKomarudinÎncă nu există evaluări
- Cool Fire Manual 45M620N2UK-01Document198 paginiCool Fire Manual 45M620N2UK-01prejby91% (11)
- Notepad++ Shortcut Keys ListDocument1 paginăNotepad++ Shortcut Keys ListWillieÎncă nu există evaluări
- Operational AmplifiersDocument35 paginiOperational AmplifierskunwarÎncă nu există evaluări
- Exploring Linux Build Systems - Buildroot Lab ManualDocument38 paginiExploring Linux Build Systems - Buildroot Lab Manualhamzamehboob103Încă nu există evaluări
- Availability and ReachabilityDocument1 paginăAvailability and ReachabilityAndre Syah FahmiÎncă nu există evaluări
- Norma JIC 37Document36 paginiNorma JIC 37guguimirandaÎncă nu există evaluări
- Steam / Power SystemDocument63 paginiSteam / Power SystemNabil SalimÎncă nu există evaluări
- Calculating Species Importance ValuesDocument3 paginiCalculating Species Importance Valuesabraha gebruÎncă nu există evaluări
- 06 Strengthening MechanismsDocument63 pagini06 Strengthening MechanismsMURALIGOCAM_29070605100% (1)
- Article - Designing Sand Cores and ToolingDocument4 paginiArticle - Designing Sand Cores and ToolingroyhanÎncă nu există evaluări
- AC 23-8B Flight Test Guide App 1Document22 paginiAC 23-8B Flight Test Guide App 1Ladislao PazmanyÎncă nu există evaluări
- 500 MCQs Computer Awarness For IBPS RRB PO (By Studyniti)Document86 pagini500 MCQs Computer Awarness For IBPS RRB PO (By Studyniti)Santosh SarswatÎncă nu există evaluări
- Examples S-Convex FunctionsDocument7 paginiExamples S-Convex Functionstradutora100% (2)
- Some Best Questions On TrigonometryDocument4 paginiSome Best Questions On TrigonometryRaghav MadanÎncă nu există evaluări
- Cam Imp (Veena)Document16 paginiCam Imp (Veena)Sidpara DeepÎncă nu există evaluări
- Handout 3 TMR4305 Lecture 13 09 2007Document5 paginiHandout 3 TMR4305 Lecture 13 09 2007sujaydsouza1987Încă nu există evaluări
- Final PPT of Carbon NanotubesDocument29 paginiFinal PPT of Carbon Nanotubesmkumar_5481450% (2)
- EE2253 - Control Systems PDFDocument124 paginiEE2253 - Control Systems PDFaduveyÎncă nu există evaluări
- K Type Thermocouple Extension Cable KXYY (1-50) Pairs X 1.5 MM 300 VDocument1 paginăK Type Thermocouple Extension Cable KXYY (1-50) Pairs X 1.5 MM 300 VArthurÎncă nu există evaluări
- ET4117 Electrical Machines and Drives Lecture5Document31 paginiET4117 Electrical Machines and Drives Lecture5farhan beighÎncă nu există evaluări
- Alkane and AlkeneDocument40 paginiAlkane and AlkenePawankumar Gupta91% (11)
- Introduction To PSpice PDFDocument7 paginiIntroduction To PSpice PDFEduardo FernándezÎncă nu există evaluări
- Georeferencing and Digitization in QGISDocument82 paginiGeoreferencing and Digitization in QGISThanosÎncă nu există evaluări
- 1 s2.0 S0960077922005665 MainDocument8 pagini1 s2.0 S0960077922005665 MainSajjad AliÎncă nu există evaluări
- Landscape Products: Technical GuideDocument124 paginiLandscape Products: Technical Guidegabbo24Încă nu există evaluări
- F2700 PDFDocument12 paginiF2700 PDFAhmad Zubair RasulyÎncă nu există evaluări
- Surge Arresters: Selection, Application and Testing: Pass YouDocument30 paginiSurge Arresters: Selection, Application and Testing: Pass YouOoi Ban JuanÎncă nu există evaluări