S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Nurse Education in Practice: Book ReviewsDocument1 paginăNurse Education in Practice: Book ReviewsUswatun HasanahÎncă nu există evaluări
- WOC CombustioDocument15 paginiWOC CombustioUswatun HasanahÎncă nu există evaluări
- Nurse Education in Practice: Book ReviewsDocument1 paginăNurse Education in Practice: Book ReviewsUswatun HasanahÎncă nu există evaluări
- Original Research: Enny Virda Yuniarti, Ima Rahmawati2Document8 paginiOriginal Research: Enny Virda Yuniarti, Ima Rahmawati2Uswatun HasanahÎncă nu există evaluări
- Pandu Tedja (938-945) - EfektivitasDocument7 paginiPandu Tedja (938-945) - EfektivitasUswatun HasanahÎncă nu există evaluări
- KW Ekke Boom 2008Document10 paginiKW Ekke Boom 2008YuliaÎncă nu există evaluări
- Serum Creatinine and Blood Urea Nitrogen Levels in Patients With Coronary Artery DiseaseDocument5 paginiSerum Creatinine and Blood Urea Nitrogen Levels in Patients With Coronary Artery DiseaseUswatun HasanahÎncă nu există evaluări
- Braden ScaleDocument1 paginăBraden ScaleRandall StevensÎncă nu există evaluări
- 67-Khoirun Nisa-Early Detection of Breast Cancer PDFDocument5 pagini67-Khoirun Nisa-Early Detection of Breast Cancer PDFUswatun HasanahÎncă nu există evaluări
- Nurse Education in Practice: Book ReviewsDocument1 paginăNurse Education in Practice: Book ReviewsUswatun HasanahÎncă nu există evaluări
- 67-Khoirun Nisa-Early Detection of Breast Cancer PDFDocument5 pagini67-Khoirun Nisa-Early Detection of Breast Cancer PDFUswatun HasanahÎncă nu există evaluări
- The Impact of Obesity On Severely Injured Children and AdolescentsDocument4 paginiThe Impact of Obesity On Severely Injured Children and AdolescentsUswatun HasanahÎncă nu există evaluări
- Individual Difference Variables and The Effects of Progressive Muscle Relaxation and Analgesic Imagery Interventions On Cancer PainDocument12 paginiIndividual Difference Variables and The Effects of Progressive Muscle Relaxation and Analgesic Imagery Interventions On Cancer PainUswatun HasanahÎncă nu există evaluări
- Thomas 2017Document8 paginiThomas 2017Uswatun HasanahÎncă nu există evaluări
- Individual Difference Variables and The Effects of Progressive Muscle Relaxation and Analgesic Imagery Interventions On Cancer PainDocument12 paginiIndividual Difference Variables and The Effects of Progressive Muscle Relaxation and Analgesic Imagery Interventions On Cancer PainUswatun HasanahÎncă nu există evaluări
- The Impact of Obesity On Severely Injured Children and AdolescentsDocument4 paginiThe Impact of Obesity On Severely Injured Children and AdolescentsUswatun HasanahÎncă nu există evaluări
- PMR AnxietyDocument19 paginiPMR AnxietyUswatun HasanahÎncă nu există evaluări
- Obesid Fisiop e Trat PDFDocument16 paginiObesid Fisiop e Trat PDFCamilla CristinaÎncă nu există evaluări
- Journal of Personality and Social Psychology VolumeDocument11 paginiJournal of Personality and Social Psychology VolumeUswatun HasanahÎncă nu există evaluări
- Niemz 2005Document9 paginiNiemz 2005Uswatun HasanahÎncă nu există evaluări
- Diagnosis of DementiaDocument6 paginiDiagnosis of DementiaUswatun Hasanah100% (1)
- Serum Creatinine and Blood Urea Nitrogen Levels in Patients With Coronary Artery DiseaseDocument5 paginiSerum Creatinine and Blood Urea Nitrogen Levels in Patients With Coronary Artery DiseaseUswatun HasanahÎncă nu există evaluări
- Associ ADHD and BullyingDocument11 paginiAssoci ADHD and BullyingUswatun HasanahÎncă nu există evaluări
- Final Dissertation PeacockDocument238 paginiFinal Dissertation PeacockUswatun HasanahÎncă nu există evaluări
- Individual Difference in Response Ro ProvocationDocument17 paginiIndividual Difference in Response Ro ProvocationUswatun HasanahÎncă nu există evaluări
- Hubungan Tingkat Ansietas Dasar Dengan Adiksi Internet Pada Pengunjung Ruang Layanan Digital Perpustakaan Universitas Sriwijaya IndralayaDocument9 paginiHubungan Tingkat Ansietas Dasar Dengan Adiksi Internet Pada Pengunjung Ruang Layanan Digital Perpustakaan Universitas Sriwijaya IndralayaUswatun HasanahÎncă nu există evaluări
- Impact of CyberbullyingDocument37 paginiImpact of CyberbullyingUswatun Hasanah100% (1)
- Insecure Attachment Attitudes in The Onset of Problematic Internet Use Among Late AdolescentsDocument9 paginiInsecure Attachment Attitudes in The Onset of Problematic Internet Use Among Late AdolescentsUswatun HasanahÎncă nu există evaluări
- Insecure Attachment Attitudes in The Onset of Problematic Internet Use Among Late AdolescentsDocument9 paginiInsecure Attachment Attitudes in The Onset of Problematic Internet Use Among Late AdolescentsUswatun HasanahÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- EpendymomaDocument5 paginiEpendymomaDenny's BerciaÎncă nu există evaluări
- Sgop CPG 2008 FinalDocument105 paginiSgop CPG 2008 FinalVia Alip100% (2)
- Bio-Data: Degree Subject Area Period of Study University / Institute Subjects From ToDocument7 paginiBio-Data: Degree Subject Area Period of Study University / Institute Subjects From ToampharmÎncă nu există evaluări
- Cracking Cancer Toolkit Slides June 19 Jeffrey Dach Mitch Ghen 2021 AA2Document97 paginiCracking Cancer Toolkit Slides June 19 Jeffrey Dach Mitch Ghen 2021 AA2André Amorim67% (3)
- Pedoman Kanker OvariumDocument31 paginiPedoman Kanker OvariumRiana SuwarniÎncă nu există evaluări
- Parameters of Care Dentoalveolar Surgery 2012Document22 paginiParameters of Care Dentoalveolar Surgery 2012api-265532519Încă nu există evaluări
- Dr. Rubi Li not liable for failure to disclose chemotherapy side effectsDocument2 paginiDr. Rubi Li not liable for failure to disclose chemotherapy side effectsBasil MaguigadÎncă nu există evaluări
- 15 Zeolite Uses & Benefits (Incl. Detox) + Side Effects - SelfhackedDocument19 pagini15 Zeolite Uses & Benefits (Incl. Detox) + Side Effects - SelfhackedtsolakidesmedÎncă nu există evaluări
- Jurnal Devia Ola YuliaDocument16 paginiJurnal Devia Ola YuliaDevia Ola YuliaÎncă nu există evaluări
- 20 Herbs That Can Fight CancerDocument6 pagini20 Herbs That Can Fight CancerahceneÎncă nu există evaluări
- Hodgkin's DiseaseDocument28 paginiHodgkin's DiseasebikeyÎncă nu există evaluări
- Cancer Patient's Guide To Overc - Derek HopkoDocument300 paginiCancer Patient's Guide To Overc - Derek HopkoGermán Edgardo MenevichianÎncă nu există evaluări
- Kalonji Benefits ImpDocument18 paginiKalonji Benefits Impjas899100% (1)
- BH3 Mimetics in AML TherapyDocument22 paginiBH3 Mimetics in AML TherapyAbhilash ReddyÎncă nu există evaluări
- 50-Year-Old Man Overcomes His Battle With Lung Cancer Using Cannabis Oil, Stuns CBS NewsDocument16 pagini50-Year-Old Man Overcomes His Battle With Lung Cancer Using Cannabis Oil, Stuns CBS Newstahirmaqpk100% (1)
- Herbotherapy and Ganotherapy Is Simply A Line of Thought Consists of Four Observation Theories Used To Explain How Ganoderma or Reishi Supports The Body Which in Turn Overcomes Its Health ProbDocument13 paginiHerbotherapy and Ganotherapy Is Simply A Line of Thought Consists of Four Observation Theories Used To Explain How Ganoderma or Reishi Supports The Body Which in Turn Overcomes Its Health Probjunver100% (1)
- Odisha Rate Contract For MedicinesDocument66 paginiOdisha Rate Contract For MedicinesSahil KargwalÎncă nu există evaluări
- PharmaceuticsDocument25 paginiPharmaceuticsvera GaborÎncă nu există evaluări
- Chapter 07 - Hematologic ProblemsDocument8 paginiChapter 07 - Hematologic ProblemscariÎncă nu există evaluări
- Comparing The ECOG Performance Status To The Karnofsky Performance StatusDocument2 paginiComparing The ECOG Performance Status To The Karnofsky Performance Statustri windartiÎncă nu există evaluări
- Therapeutics Handbook 2014 - 140804Document384 paginiTherapeutics Handbook 2014 - 140804Eriet HidayatÎncă nu există evaluări
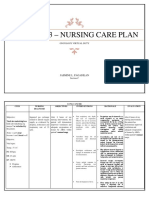
- Activity 3 - Nursing Care Plan: Oncology Virtual DutyDocument9 paginiActivity 3 - Nursing Care Plan: Oncology Virtual DutyAngelica Charisse BuliganÎncă nu există evaluări
- A New Treatment Method of Advanced Metastic TumorsDocument7 paginiA New Treatment Method of Advanced Metastic TumorsDiana DíazÎncă nu există evaluări
- Oncologic NRSG NotesDocument13 paginiOncologic NRSG NotesMigo LuisÎncă nu există evaluări
- Intel STS Semifinalists 2016Document32 paginiIntel STS Semifinalists 2016BayAreaNewsGroupÎncă nu există evaluări
- Oncology NotesDocument7 paginiOncology Notesaurezea100% (1)
- Chitosan Nanoparticles PHD ThesisDocument6 paginiChitosan Nanoparticles PHD Thesisfjgmmmew100% (2)
- 2015 The Influence of Gut Microbiota On Drug Metabolism and Toxicity. EODMTDocument29 pagini2015 The Influence of Gut Microbiota On Drug Metabolism and Toxicity. EODMTJoseloÎncă nu există evaluări
- The Treatment of Stage IV CancersDocument6 paginiThe Treatment of Stage IV CancersAnthony SullivanÎncă nu există evaluări
- Neoplastic DisordersDocument36 paginiNeoplastic DisordersJSeasharkÎncă nu există evaluări