S-ar putea să vă placă și
- Fgdcnhgjkhkijuolpujkjgj MHGNH GfbgfdtgbdfvsdrfdswredawfrDocument1 paginăFgdcnhgjkhkijuolpujkjgj MHGNH GfbgfdtgbdfvsdrfdswredawfrIntania RosatiÎncă nu există evaluări
- KHVFJGFHGDocument1 paginăKHVFJGFHGIntania RosatiÎncă nu există evaluări
- Cataract Senilis Matur Od: Intania Rosati H1A013031 Supervisor: Dr. Siti Farida, SP.M (K)Document23 paginiCataract Senilis Matur Od: Intania Rosati H1A013031 Supervisor: Dr. Siti Farida, SP.M (K)Intania RosatiÎncă nu există evaluări
- ShbfvemrgfhrgdfjDocument1 paginăShbfvemrgfhrgdfjIntania RosatiÎncă nu există evaluări
- lSFHKwebaifkbkuyvbkaeyrfgkuefgkuyfgkaeygaluirefkudhgujhg lSFHKwebaifkbkuyvbkaeyrfgkuefgkuyfgkaeygaluirefkudhgujhgDocument1 paginălSFHKwebaifkbkuyvbkaeyrfgkuefgkuyfgkaeygaluirefkudhgujhg lSFHKwebaifkbkuyvbkaeyrfgkuefgkuyfgkaeygaluirefkudhgujhgIntania RosatiÎncă nu există evaluări
- JHSBCJDocument1 paginăJHSBCJIntania RosatiÎncă nu există evaluări
- SjhvcjsdhgcnsugdyfmufhgmikrfjhcdDocument1 paginăSjhvcjsdhgcnsugdyfmufhgmikrfjhcdIntania RosatiÎncă nu există evaluări
- lSFHKwebaifkbkuyvbkaeyrfgkuefgkuyfgkaeygaluirefkudhgujhg lSFHKwebaifkbkuyvbkaeyrfgkuefgkuyfgkaeygaluirefkudhgujhgDocument1 paginălSFHKwebaifkbkuyvbkaeyrfgkuefgkuyfgkaeygaluirefkudhgujhg lSFHKwebaifkbkuyvbkaeyrfgkuefgkuyfgkaeygaluirefkudhgujhgIntania RosatiÎncă nu există evaluări
- BMI Asia PDFDocument12 paginiBMI Asia PDFBunda KiaraÎncă nu există evaluări
- JTDGNFDocument1 paginăJTDGNFIntania RosatiÎncă nu există evaluări
- KHVFJGFHGDocument1 paginăKHVFJGFHGIntania RosatiÎncă nu există evaluări
- JGCMHGCDocument29 paginiJGCMHGCIntania RosatiÎncă nu există evaluări
- Dhony Kartika Nugroho, Pudjiatmoko, Diarmitha IK, Tum S, Schoonman LDocument5 paginiDhony Kartika Nugroho, Pudjiatmoko, Diarmitha IK, Tum S, Schoonman LIntania RosatiÎncă nu există evaluări
- Adnexa Mass N pregnancyEDitDocument18 paginiAdnexa Mass N pregnancyEDitIntania RosatiÎncă nu există evaluări
- FGNBFCXBGDocument5 paginiFGNBFCXBGIntania RosatiÎncă nu există evaluări
- Adnexa Mass N pregnancyEDitDocument18 paginiAdnexa Mass N pregnancyEDitIntania RosatiÎncă nu există evaluări
- Journal of Forensic and Legal Medicine: Cristian D'Ovidio, Enrica Rosato, Aldo CarnevaleDocument4 paginiJournal of Forensic and Legal Medicine: Cristian D'Ovidio, Enrica Rosato, Aldo CarnevaleIntania RosatiÎncă nu există evaluări
- Cover Blok XXDocument1 paginăCover Blok XXIntania RosatiÎncă nu există evaluări
- Risk Factors for Cervical Cancer StudyDocument7 paginiRisk Factors for Cervical Cancer StudyIntania RosatiÎncă nu există evaluări
- 330 639 1 SMDocument6 pagini330 639 1 SMDimes Atika PermanasariÎncă nu există evaluări
- Risk Factors For Cardiovascular Disease in Women: Assessment and ManagementDocument7 paginiRisk Factors For Cardiovascular Disease in Women: Assessment and ManagementIntania RosatiÎncă nu există evaluări
- Prolonged LaborDocument32 paginiProlonged LaborIntania RosatiÎncă nu există evaluări
- Reoccurance HypertentionDocument17 paginiReoccurance HypertentionIntania RosatiÎncă nu există evaluări
- Pneumonia Case: Bad Oeynhausen 2012-1Document4 paginiPneumonia Case: Bad Oeynhausen 2012-1Intania RosatiÎncă nu există evaluări
- Hiperemesiss GravidarumDocument15 paginiHiperemesiss GravidarumIntania RosatiÎncă nu există evaluări
- Dhony Kartika Nugroho, Pudjiatmoko, Diarmitha IK, Tum S, Schoonman LDocument5 paginiDhony Kartika Nugroho, Pudjiatmoko, Diarmitha IK, Tum S, Schoonman LIntania RosatiÎncă nu există evaluări
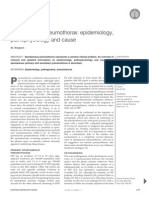
- Spontan PneumothoraxDocument3 paginiSpontan PneumothoraxSuriyani SofianÎncă nu există evaluări
- Adnexal Mass in Pregnancy: Ario DaniantoDocument18 paginiAdnexal Mass in Pregnancy: Ario DaniantoIntania RosatiÎncă nu există evaluări
- Bahan IKMDocument18 paginiBahan IKMRifqiÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Red Velvet Cake RecipeDocument6 paginiRed Velvet Cake RecipeRuminto SubektiÎncă nu există evaluări
- Home Study Report of Resident Indian Parent: Name of The Social WorkerDocument4 paginiHome Study Report of Resident Indian Parent: Name of The Social WorkerVmksÎncă nu există evaluări
- Geoheritage of Labuan Island: Bulletin of The Geological Society of Malaysia December 2016Document14 paginiGeoheritage of Labuan Island: Bulletin of The Geological Society of Malaysia December 2016songkkÎncă nu există evaluări
- Butterfly Valve ConcentricDocument6 paginiButterfly Valve ConcentricpramodtryÎncă nu există evaluări
- Msae Msae2018-Arwm012 Full Dronespraying 2Document4 paginiMsae Msae2018-Arwm012 Full Dronespraying 2Muhammad Huzaifah Mohd RoslimÎncă nu există evaluări
- ITC's diverse businesses: cigarettes, packaging, hotels, paperboards, stationery, matches, incense sticks, retail, food, exportsDocument1 paginăITC's diverse businesses: cigarettes, packaging, hotels, paperboards, stationery, matches, incense sticks, retail, food, exportsShashank JainÎncă nu există evaluări
- Recent Developments in Carbapenems: ReviewDocument16 paginiRecent Developments in Carbapenems: ReviewFrancielleÎncă nu există evaluări
- CAP - 5 - 54. Billions and Billions of Demons - by Richard C. Lewontin - The New York Review of BooksDocument11 paginiCAP - 5 - 54. Billions and Billions of Demons - by Richard C. Lewontin - The New York Review of BooksRaimundo Filho100% (1)
- ECD KEBVF5 Installation ManualDocument32 paginiECD KEBVF5 Installation Manualashish gautamÎncă nu există evaluări
- Electro BladeDocument2 paginiElectro Bladeapi-19808945Încă nu există evaluări
- Whats That TreeDocument2 paginiWhats That Treeapi-223191715100% (1)
- Handout2 Fischer CarbeneDocument5 paginiHandout2 Fischer CarbeneMuhammad ShimaÎncă nu există evaluări
- Low Back Pain Anatomy of Thoracolumbar SpineDocument10 paginiLow Back Pain Anatomy of Thoracolumbar SpineMÎncă nu există evaluări
- Nigeria Trainers ManualDocument131 paginiNigeria Trainers ManualVivi ALÎncă nu există evaluări
- Food Salt: By: Saad, Rehan, Asad, Hasan, Adil, Abdur Rehman, AzharDocument10 paginiFood Salt: By: Saad, Rehan, Asad, Hasan, Adil, Abdur Rehman, AzharsaadÎncă nu există evaluări
- Numerical Modelling of Drying Kinetics of Banana Flower Using Natural and Forced Convection DryersDocument5 paginiNumerical Modelling of Drying Kinetics of Banana Flower Using Natural and Forced Convection DryersMuthu KumarÎncă nu există evaluări
- Guidance Counseling EssentialsDocument2 paginiGuidance Counseling EssentialsElizabeth E. FetizaÎncă nu există evaluări
- Fault Location of Overhead Transmission Line With Noncontact Magnetic Field MeasurementDocument10 paginiFault Location of Overhead Transmission Line With Noncontact Magnetic Field MeasurementJkÎncă nu există evaluări
- 10893259-PIB 背钳弹簧保持架垫片落物事件Document2 pagini10893259-PIB 背钳弹簧保持架垫片落物事件xlzyydf2015Încă nu există evaluări
- CuO Based Solar Cell With V2O5 BSF Layer - Theoretical Validation of Experimental DataDocument12 paginiCuO Based Solar Cell With V2O5 BSF Layer - Theoretical Validation of Experimental DataNur Aisyah ShariÎncă nu există evaluări
- Certificate of Analysis: Ship Date: Port of Discharge: Carrier: Vessel: Voyage: Quantity (MT) : Us GallonsDocument1 paginăCertificate of Analysis: Ship Date: Port of Discharge: Carrier: Vessel: Voyage: Quantity (MT) : Us GallonsMercadeo BelaraviÎncă nu există evaluări
- ABO BLOOD GROUP Part 1Document104 paginiABO BLOOD GROUP Part 1Taladua Cayla Grace O.Încă nu există evaluări
- HVAC Report FINALDocument65 paginiHVAC Report FINALIanÎncă nu există evaluări
- Pre Mocks Y11 2023Document14 paginiPre Mocks Y11 2023Ahsan AhmedÎncă nu există evaluări
- ICH Topic Q 3 B (R2) Impurities in New Drug Products: European Medicines AgencyDocument14 paginiICH Topic Q 3 B (R2) Impurities in New Drug Products: European Medicines AgencyJesus Barcenas HernandezÎncă nu există evaluări
- Guerra, Germae Joyce - Media JournalDocument2 paginiGuerra, Germae Joyce - Media JournalGERMAE JOYCE GUERRAÎncă nu există evaluări
- Commercial Inverter AC Service ManualDocument116 paginiCommercial Inverter AC Service ManualEdwin JaramilloÎncă nu există evaluări
- Physical Science - q3 - Slm3Document15 paginiPhysical Science - q3 - Slm3Boyet Alvarez AtibagosÎncă nu există evaluări
- Cap Dev Dimalinao 2023-2027Document4 paginiCap Dev Dimalinao 2023-2027CA T HeÎncă nu există evaluări
- Final Draft - Banana ChipsDocument34 paginiFinal Draft - Banana ChipsAubrey Delgado74% (35)