S-ar putea să vă placă și
- Biopolymer Electrolytes: Fundamentals and Applications in Energy StorageDe la EverandBiopolymer Electrolytes: Fundamentals and Applications in Energy StorageÎncă nu există evaluări
- Termpaper 214bm1381 4thsemDocument5 paginiTermpaper 214bm1381 4thsemVeena VyasÎncă nu există evaluări
- NANOTECHNOLOGY REVIEW: LIPOSOMES, NANOTUBES & PLGA NANOPARTICLESDe la EverandNANOTECHNOLOGY REVIEW: LIPOSOMES, NANOTUBES & PLGA NANOPARTICLESÎncă nu există evaluări
- BME 463 LECTURE 1bDocument19 paginiBME 463 LECTURE 1bKOFI BROWNÎncă nu există evaluări
- Classes of Materials Used in Medicine: 4/1/2020 Done By: Dr. Amani Al-Ghraibah Al-Ahliyya Amman UniversityDocument14 paginiClasses of Materials Used in Medicine: 4/1/2020 Done By: Dr. Amani Al-Ghraibah Al-Ahliyya Amman UniversityMOHAMMAD AKEFÎncă nu există evaluări
- Degradation of Materials in The Biological Environment: SectionDocument2 paginiDegradation of Materials in The Biological Environment: SectionZohaib Khurshid SultanÎncă nu există evaluări
- Biodegradable PolymersDocument7 paginiBiodegradable PolymersArchit GuptaÎncă nu există evaluări
- Uso Pom 2 PDFDocument7 paginiUso Pom 2 PDFLauMarquezÎncă nu există evaluări
- Biomedical Polymers: B.Sc. Project ReportDocument19 paginiBiomedical Polymers: B.Sc. Project ReportPaulami Bose90% (10)
- Biodegradable PolymersDocument16 paginiBiodegradable PolymersAnonymous oSJ15KEc100% (1)
- Research Paper 1Document15 paginiResearch Paper 1Puru GaurÎncă nu există evaluări
- Characters of PolymersDocument3 paginiCharacters of PolymerstariqjiyaÎncă nu există evaluări
- Non-Hydrolyzable Plastics - An Interdisciplinary Look at Plastic Bio-OxidationDocument12 paginiNon-Hydrolyzable Plastics - An Interdisciplinary Look at Plastic Bio-Oxidationtiffany charlottaÎncă nu există evaluări
- The Essential Role of Hydrodynamic Shear Force in The Formation of Biofilm and Granular SludgeDocument13 paginiThe Essential Role of Hydrodynamic Shear Force in The Formation of Biofilm and Granular SludgeRicardo BrandãoÎncă nu există evaluări
- 0001 UNIT-I NotesproDocument34 pagini0001 UNIT-I Notesprokishan kumarÎncă nu există evaluări
- Surface Modification of Polymers For Biomedical ApplicationsDocument8 paginiSurface Modification of Polymers For Biomedical ApplicationspcnferreiraÎncă nu există evaluări
- Biodegradation of Poly (Lactic Acid) - Chitosan Stratified Composites in PDFDocument12 paginiBiodegradation of Poly (Lactic Acid) - Chitosan Stratified Composites in PDFIrina PaslaruÎncă nu există evaluări
- Designing HydrogelDocument38 paginiDesigning Hydrogeljuleslee1234Încă nu există evaluări
- Self Healing Composite MaterialsDocument55 paginiSelf Healing Composite MaterialsWebsoft Tech-HydÎncă nu există evaluări
- Biopolymer Technology and ApplicationsDocument24 paginiBiopolymer Technology and ApplicationsXuan PhuongÎncă nu există evaluări
- New Advancements of Bioplastics in Medical ApplicationsDocument15 paginiNew Advancements of Bioplastics in Medical ApplicationsBrizeth García DíazÎncă nu există evaluări
- Biocide Techn 4ppDocument4 paginiBiocide Techn 4ppeduardoÎncă nu există evaluări
- Ajbsr MS Id 001682Document9 paginiAjbsr MS Id 001682sjonathanpastorÎncă nu există evaluări
- 4 Hydrogels in Drug DeliveryDocument15 pagini4 Hydrogels in Drug Deliveryblueflame9505050% (2)
- Biomedical Applications of Polymers - An: Mini ReviewDocument2 paginiBiomedical Applications of Polymers - An: Mini Reviewاسلام غازي ذياب احمدÎncă nu există evaluări
- Silk Fibroinchitosanalginate Multilayer Membranes As A System For Controlled Drug Release in Wound HealingDocument9 paginiSilk Fibroinchitosanalginate Multilayer Membranes As A System For Controlled Drug Release in Wound HealingвикторÎncă nu există evaluări
- Biomaterials and BiocompatibiltDocument34 paginiBiomaterials and Biocompatibiltsindy mÎncă nu există evaluări
- Hydrogels in Drug Delivery - Progress and ChallengesDocument15 paginiHydrogels in Drug Delivery - Progress and ChallengesЕгор ЛетовÎncă nu există evaluări
- BioestimuladoresDocument4 paginiBioestimuladoresLaís CanhoniÎncă nu există evaluări
- Water Soluble Polymer Flocculants Synthesis, PDFDocument43 paginiWater Soluble Polymer Flocculants Synthesis, PDFruizgj2011Încă nu există evaluări
- BiodegradationDocument3 paginiBiodegradationBhoomika HollaÎncă nu există evaluări
- Reverse Osmosis State of The Art in IndonesiaDocument16 paginiReverse Osmosis State of The Art in IndonesiachrisÎncă nu există evaluări
- Biodegradable Polymers - Investigatory ProjectDocument28 paginiBiodegradable Polymers - Investigatory ProjectHuzaifaÎncă nu există evaluări
- Scaffolds in Tissue Engineering Bone and Cartilage PDFDocument15 paginiScaffolds in Tissue Engineering Bone and Cartilage PDFNhật TùngÎncă nu există evaluări
- APS - TEMED ReactionDocument11 paginiAPS - TEMED ReactionMichiko MatsuoÎncă nu există evaluări
- Bioresorbable MaterialsDocument40 paginiBioresorbable MaterialssaurabhsriÎncă nu există evaluări
- Tissue Engineering SummaryDocument28 paginiTissue Engineering SummaryDwisetyaSafirnaWidyaratihÎncă nu există evaluări
- New Perspectives in Plastic Biodegradation PDFDocument6 paginiNew Perspectives in Plastic Biodegradation PDFCristina RangelÎncă nu există evaluări
- Swellable MatricesDocument7 paginiSwellable MatricesvyÎncă nu există evaluări
- Biodegradable Polymers, Medical ApplicationsDocument23 paginiBiodegradable Polymers, Medical ApplicationsCaroline LidyaÎncă nu există evaluări
- 04JBT 1243Document9 pagini04JBT 1243Mousam ChoudhuryÎncă nu există evaluări
- Microbial Degradation Polyethylene - 2014Document9 paginiMicrobial Degradation Polyethylene - 2014Lednys Palomino ZambranoÎncă nu există evaluări
- Biodegradable Intelligent' Materials in Response To Physical Stimuli For Biomedical ApplicationsDocument15 paginiBiodegradable Intelligent' Materials in Response To Physical Stimuli For Biomedical ApplicationsNguyễn Quốc HiệqÎncă nu există evaluări
- Electrochemically Assisted Deposition of Biodegradable Polymer Nanoparticles/ Sol-Gel Thin FilmsDocument6 paginiElectrochemically Assisted Deposition of Biodegradable Polymer Nanoparticles/ Sol-Gel Thin FilmsVikas PatilÎncă nu există evaluări
- Surfacebulk PDFDocument11 paginiSurfacebulk PDFVishwarup GoswamiÎncă nu există evaluări
- A Mini-Review On Membrane FoulingDocument8 paginiA Mini-Review On Membrane FoulingManukoArteagaÎncă nu există evaluări
- HYDROGEL : A SMART POLYMER: AN OVERVIEW Ganesh Bamane*, Tejaswini Kakade, Akash Raval, Prasad Kevane, Sucheta Tikole MSS’College of Pharmacy Medha, Tal-Jaoli, Dist –Satara, India. YSPM’S, YTC, Faculty of Pharmacy, Satara, India.Document29 paginiHYDROGEL : A SMART POLYMER: AN OVERVIEW Ganesh Bamane*, Tejaswini Kakade, Akash Raval, Prasad Kevane, Sucheta Tikole MSS’College of Pharmacy Medha, Tal-Jaoli, Dist –Satara, India. YSPM’S, YTC, Faculty of Pharmacy, Satara, India.Ijupbs IjupbsÎncă nu există evaluări
- Membranes 09 00111Document81 paginiMembranes 09 00111alang_businessÎncă nu există evaluări
- Biodegradable Polymers FinalDocument38 paginiBiodegradable Polymers Finalanupnakat100% (1)
- Biomedical Applications of Biodegradable PolymersDocument63 paginiBiomedical Applications of Biodegradable PolymersSubhash SinhaÎncă nu există evaluări
- 24 Print Tan2013Document11 pagini24 Print Tan2013Noer IskhanÎncă nu există evaluări
- BT503 Environment Biotechnology (Merget PPT Handouts (1 To 235) Full Mid and Final)Document139 paginiBT503 Environment Biotechnology (Merget PPT Handouts (1 To 235) Full Mid and Final)laibaÎncă nu există evaluări
- ChitosanDocument52 paginiChitosanMrSomnambululÎncă nu există evaluări
- Polycaprolactone/starch Composite: Fabrication, Structure, Properties, and ApplicationsDocument18 paginiPolycaprolactone/starch Composite: Fabrication, Structure, Properties, and ApplicationsJOHNDELLE ROXASÎncă nu există evaluări
- Humidity-Triggered Self-Healing of Microporous Polyelectrolyte Multilayer Coatings For Hydrophobic Drug DeliveryDocument8 paginiHumidity-Triggered Self-Healing of Microporous Polyelectrolyte Multilayer Coatings For Hydrophobic Drug Delivery박수카Încă nu există evaluări
- Seminar On Biodegradable PolymersDocument19 paginiSeminar On Biodegradable Polymerskeyur33% (3)
- Bioceramics For Hard Tissue Engineering Applications: A ReviewDocument9 paginiBioceramics For Hard Tissue Engineering Applications: A ReviewAjanth PraveenÎncă nu există evaluări
- B. Pharm. Final Year (2010-11), Project ReportDocument4 paginiB. Pharm. Final Year (2010-11), Project ReportHimanshu JindalÎncă nu există evaluări
- Polymer: Alireza Shaabani, Roya SedghiDocument15 paginiPolymer: Alireza Shaabani, Roya SedghiSiddhesh Umesh MestryÎncă nu există evaluări
- Biofilm Review2004Document15 paginiBiofilm Review2004LongBien TrinhÎncă nu există evaluări
- TOEFL Faq Skilled Migration HP Ac AdaDocument11 paginiTOEFL Faq Skilled Migration HP Ac AdaDanielGonzalezÎncă nu există evaluări
- TOEFL Testmap PDFDocument1 paginăTOEFL Testmap PDFyaxuriÎncă nu există evaluări
- Floudas, C.A. Nonlinear and Mixed-Integer Optimization. Fundamentals and Applications. OxfordDocument24 paginiFloudas, C.A. Nonlinear and Mixed-Integer Optimization. Fundamentals and Applications. OxfordDanielGonzalezÎncă nu există evaluări
- TOEFL Faq Skilled Migration HP Ac AdaDocument11 paginiTOEFL Faq Skilled Migration HP Ac AdaDanielGonzalezÎncă nu există evaluări
- Edwards2004 FTIR Raman Collagen PDFDocument8 paginiEdwards2004 FTIR Raman Collagen PDFDanielGonzalezÎncă nu există evaluări
- EIS Recubrimientos 1995Document28 paginiEIS Recubrimientos 1995DanielGonzalezÎncă nu există evaluări
- EqcmDocument11 paginiEqcmDanielGonzalezÎncă nu există evaluări
- Voinova2002 Missing Mass PDFDocument7 paginiVoinova2002 Missing Mass PDFDanielGonzalezÎncă nu există evaluări
- Vieira2014 Mejoramiento A La Inflamacion PDFDocument8 paginiVieira2014 Mejoramiento A La Inflamacion PDFDanielGonzalezÎncă nu există evaluări
- PFD Version FinalDocument1 paginăPFD Version FinalDanielGonzalezÎncă nu există evaluări
- Collagen Animal Sources and Biomedical ApplicationDocument5 paginiCollagen Animal Sources and Biomedical ApplicationDanielGonzalezÎncă nu există evaluări
- Reologia de STEFFEDocument428 paginiReologia de STEFFESarai SierraÎncă nu există evaluări
- Proceso SlurryDocument8 paginiProceso SlurryDanielGonzalezÎncă nu există evaluări
- Naidoo Comparative 2013Document122 paginiNaidoo Comparative 2013DanielGonzalezÎncă nu există evaluări
- The Williams Dictionary of Biomaterials David F WiDocument1 paginăThe Williams Dictionary of Biomaterials David F WiDanielGonzalezÎncă nu există evaluări
- Rutas Del Proceso y Economia PolietilenoDocument23 paginiRutas Del Proceso y Economia PolietilenoDanielGonzalezÎncă nu există evaluări
- TP32Document39 paginiTP32saimaabdulrasheedÎncă nu există evaluări
- Production of PolyethyleneDocument13 paginiProduction of Polyethylenetokiin100% (4)
- Barnes - A Handbook of Elementary RheologyDocument210 paginiBarnes - A Handbook of Elementary RheologyXristoforos KolomvosÎncă nu există evaluări
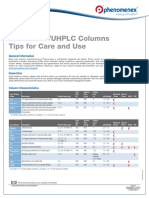
- Luna HPLC/UHPLC Columns Tips For Care and Use: General InformationDocument3 paginiLuna HPLC/UHPLC Columns Tips For Care and Use: General Informationsilfhany fatokhizarÎncă nu există evaluări
- Stream Flow Measurement Sample Report 069BCE16Document21 paginiStream Flow Measurement Sample Report 069BCE16Gaurab TimilaÎncă nu există evaluări
- Theory of Structures With AnswersDocument17 paginiTheory of Structures With AnswersJoshua OrcalesÎncă nu există evaluări
- Stem 006 Day 3Document10 paginiStem 006 Day 3Caryl Ann C. SernadillaÎncă nu există evaluări
- SPOTIFYDocument6 paginiSPOTIFYAj AntonioÎncă nu există evaluări
- Sci9 Q2 Summative-4Document6 paginiSci9 Q2 Summative-4Lanie BuenavistaÎncă nu există evaluări
- Biodiesel Production PaperDocument30 paginiBiodiesel Production PaperCarlosÎncă nu există evaluări
- Frisken 2001Document5 paginiFrisken 2001Otávio Do Couto VellozoÎncă nu există evaluări
- Physics Challenge For Teachers and Students: Cash or Charge?Document2 paginiPhysics Challenge For Teachers and Students: Cash or Charge?jerryÎncă nu există evaluări
- Exercise 5 Organic Components: Proteins and LipidsDocument2 paginiExercise 5 Organic Components: Proteins and LipidsHanna Joy BringuelaÎncă nu există evaluări
- Gas Treating Products and Services PDFDocument16 paginiGas Treating Products and Services PDFProcess EngineerÎncă nu există evaluări
- ME663 Assignment 1Document2 paginiME663 Assignment 1thanhtam3819Încă nu există evaluări
- EMF ExercisesDocument42 paginiEMF ExercisesBEEMI REDDY VENKATA REDDYÎncă nu există evaluări
- Universal CGPA Calculator For EEEDocument16 paginiUniversal CGPA Calculator For EEEG2zapper gamingÎncă nu există evaluări
- Presentation Stage 1Document13 paginiPresentation Stage 1Khushi UdasiÎncă nu există evaluări
- Helicopter Maintenance Magazine Apr-May 2023Document32 paginiHelicopter Maintenance Magazine Apr-May 2023Jose A. HerreraÎncă nu există evaluări
- MonevaDocument15 paginiMonevaKurt Lester Moneva100% (1)
- Bearing Materials - Engineering Materials & Metallurgy Questions and Answers - SanfoundryDocument3 paginiBearing Materials - Engineering Materials & Metallurgy Questions and Answers - SanfoundrySample UseÎncă nu există evaluări
- Alkaloids AvnishDocument16 paginiAlkaloids AvnishDr. Avnish Upadhyay100% (22)
- The Art of Scientific Writing and Ethical Use of Artificial IntelligenceDocument18 paginiThe Art of Scientific Writing and Ethical Use of Artificial IntelligenceHaroon RashidÎncă nu există evaluări
- A2 Entropy NotesDocument16 paginiA2 Entropy NotesZim Ahmed ZavianÎncă nu există evaluări
- Agglomeration PracticeDocument57 paginiAgglomeration Practiceabdulloh_99Încă nu există evaluări
- m2 Lab - Gravitational Forces Sim-2Document6 paginim2 Lab - Gravitational Forces Sim-2api-309607575Încă nu există evaluări
- 20 Electrostatics-Coulomb's LawDocument5 pagini20 Electrostatics-Coulomb's Laweltytan50% (2)
- Mil DTL 46027KDocument28 paginiMil DTL 46027KRobertÎncă nu există evaluări
- 20200414014739976f2ee727 1Document12 pagini20200414014739976f2ee727 1Ram RathiyaÎncă nu există evaluări
- WorkshopSolarRoofTop DonBoscoSumbaDocument75 paginiWorkshopSolarRoofTop DonBoscoSumbaDominggus TelupunÎncă nu există evaluări
- CATALISEDocument13 paginiCATALISEANTONIO RAUL MANUELÎncă nu există evaluări
- Dodecatemoria - FirmicusDocument3 paginiDodecatemoria - FirmicusMihaela Dicu100% (1)
- Movie Review of Interstellar by Christopher Nolan Plot Characters and VisualsDocument3 paginiMovie Review of Interstellar by Christopher Nolan Plot Characters and VisualsRekha DhoundiyalÎncă nu există evaluări
- The Obesity Code: Unlocking the Secrets of Weight LossDe la EverandThe Obesity Code: Unlocking the Secrets of Weight LossEvaluare: 4 din 5 stele4/5 (6)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDe la EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsÎncă nu există evaluări
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeEvaluare: 2 din 5 stele2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe la EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityEvaluare: 4 din 5 stele4/5 (24)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDe la EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDe la EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisEvaluare: 4.5 din 5 stele4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDe la EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedEvaluare: 5 din 5 stele5/5 (80)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDe la EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDEvaluare: 5 din 5 stele5/5 (1)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!De la EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Evaluare: 5 din 5 stele5/5 (1)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDe la EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsEvaluare: 5 din 5 stele5/5 (1)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDe la EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisEvaluare: 4 din 5 stele4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.De la EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Evaluare: 4.5 din 5 stele4.5/5 (110)
- Gut: the new and revised Sunday Times bestsellerDe la EverandGut: the new and revised Sunday Times bestsellerEvaluare: 4 din 5 stele4/5 (392)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDe la EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityEvaluare: 4 din 5 stele4/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDe la EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsEvaluare: 4.5 din 5 stele4.5/5 (169)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDe la EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryEvaluare: 4 din 5 stele4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDe la EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessEvaluare: 4.5 din 5 stele4.5/5 (328)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDe la EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsEvaluare: 3.5 din 5 stele3.5/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisDe la EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisEvaluare: 3.5 din 5 stele3.5/5 (2)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningDe la EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningEvaluare: 4 din 5 stele4/5 (3)
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)De la EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Evaluare: 4 din 5 stele4/5 (378)
- To Explain the World: The Discovery of Modern ScienceDe la EverandTo Explain the World: The Discovery of Modern ScienceEvaluare: 3.5 din 5 stele3.5/5 (51)
- The Marshmallow Test: Mastering Self-ControlDe la EverandThe Marshmallow Test: Mastering Self-ControlEvaluare: 4.5 din 5 stele4.5/5 (58)