S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Medical Coding 1 - ExamDocument4 paginiMedical Coding 1 - ExamAnthony Martinez75% (4)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Tonsillectomy Slides 050427Document62 paginiTonsillectomy Slides 050427Aidiel FikriÎncă nu există evaluări
- WSH guidelines diagnose manage occupational diseasesDocument106 paginiWSH guidelines diagnose manage occupational diseasesmediaaprina100% (1)
- Krohn Vs CA G.R. No. 108854Document2 paginiKrohn Vs CA G.R. No. 108854Francise Mae Montilla MordenoÎncă nu există evaluări
- Goal:: Ineffective Airway Clearance Related To Cumulation of SecretionDocument4 paginiGoal:: Ineffective Airway Clearance Related To Cumulation of SecretionWyen CabatbatÎncă nu există evaluări
- HIV and PregnancyDocument2 paginiHIV and PregnancyMagdalena Dwiyani HutajuluÎncă nu există evaluări
- Determining Nursing Care HoursDocument2 paginiDetermining Nursing Care HoursBambangSujanaÎncă nu există evaluări
- PERINATAL PATIENT SAFETY: Management of Oxytocin For Labor Induction and Augmentation MCN, The American Journal of Maternal/Child NursingDocument2 paginiPERINATAL PATIENT SAFETY: Management of Oxytocin For Labor Induction and Augmentation MCN, The American Journal of Maternal/Child NursingNishaThakuriÎncă nu există evaluări
- SOAP Handout 2010Document4 paginiSOAP Handout 2010wawanÎncă nu există evaluări
- 6 - Fabrication of An Implant-Supported Overdenture Using CAD-CAM Technology A Clinical ReportDocument8 pagini6 - Fabrication of An Implant-Supported Overdenture Using CAD-CAM Technology A Clinical ReportkochikaghochiÎncă nu există evaluări
- Assam Tea Gardens Cachar, Burtoll T.E. Commissionerate of Labour, Government of Assam Plantation Association name: TAIBVBDocument4 paginiAssam Tea Gardens Cachar, Burtoll T.E. Commissionerate of Labour, Government of Assam Plantation Association name: TAIBVBAvijitSinharoyÎncă nu există evaluări
- Introduction To AnesthesiologyDocument68 paginiIntroduction To AnesthesiologyOzza AlhudaÎncă nu există evaluări
- 07 - 260CME-Clinical Manifestations of Ocular TuberculosisDocument5 pagini07 - 260CME-Clinical Manifestations of Ocular TuberculosisPika LubisÎncă nu există evaluări
- Peads - Diamond Blackfan AnemiaDocument40 paginiPeads - Diamond Blackfan AnemiaBaran PalanimuthuÎncă nu există evaluări
- Chron Skin Allergy Oct 2010Document32 paginiChron Skin Allergy Oct 2010shannon3458Încă nu există evaluări
- Daptomycin (Cubicin)Document1 paginăDaptomycin (Cubicin)Adrianne BazoÎncă nu există evaluări
- Baby Gap: The Surprising Truth About America's Infant-Mortality RateDocument2 paginiBaby Gap: The Surprising Truth About America's Infant-Mortality RateJoseph AltmannÎncă nu există evaluări
- Edoc - Pub Community Health Nursing Notes SummaryDocument9 paginiEdoc - Pub Community Health Nursing Notes SummarySHAH BAZÎncă nu există evaluări
- Dr. Steven Corwin LetterDocument2 paginiDr. Steven Corwin LetterJonathan LaMantiaÎncă nu există evaluări
- NeuVision 900 Operation+ManualDocument169 paginiNeuVision 900 Operation+ManualRafael Salazar100% (1)
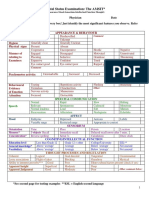
- Mental Status Examination: The AMSIT : Neat and Tidy DisshevelledDocument2 paginiMental Status Examination: The AMSIT : Neat and Tidy Disshevellednisreen100% (1)
- Group 7Document49 paginiGroup 7Muhammad Masoom AkhtarÎncă nu există evaluări
- USP CommentDocument49 paginiUSP CommentMajdi Hasan AyoubÎncă nu există evaluări
- Abstract Book 2004Document250 paginiAbstract Book 2004kindoicciÎncă nu există evaluări
- ISONIAZIDDocument2 paginiISONIAZIDPoet POet PoEtÎncă nu există evaluări
- PericarditisDocument11 paginiPericarditisrbarcellonaÎncă nu există evaluări
- TriageDocument42 paginiTriageNic JiÎncă nu există evaluări
- Adult Grip Strength Norms For The Baseline Digital DynamometerDocument25 paginiAdult Grip Strength Norms For The Baseline Digital DynamometerOmar Escalante DíazÎncă nu există evaluări
- Assessing Body TemperatureDocument6 paginiAssessing Body TemperatureemailÎncă nu există evaluări
- Nurs FPX 4020 Assessment 2 Root Cause Analysis and Safety Improvement PlanDocument5 paginiNurs FPX 4020 Assessment 2 Root Cause Analysis and Safety Improvement PlanEmma WatsonÎncă nu există evaluări