S-ar putea să vă placă și
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Zastita Od Jonizirajuceg Zracenja-Ful Tekst-94-101Document8 paginiZastita Od Jonizirajuceg Zracenja-Ful Tekst-94-101Meris JugadorÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Age Prediction in The Adult Based On The Pulp-to-Tooth Ratio in Lower Third Molars: A Cone-Beam CT StudyDocument6 paginiAge Prediction in The Adult Based On The Pulp-to-Tooth Ratio in Lower Third Molars: A Cone-Beam CT StudyMeris JugadorÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- Molina 2020Document6 paginiMolina 2020Meris JugadorÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Sujatha 2017Document9 paginiSujatha 2017Meris JugadorÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- 08 Nikolic-PundaDocument3 pagini08 Nikolic-PundaMeris JugadorÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Dental Cone Beam Computed Tomography in Children Clinical Effectiveness and Cancer Risk Due To Radiation Exposure 2019Document6 paginiDental Cone Beam Computed Tomography in Children Clinical Effectiveness and Cancer Risk Due To Radiation Exposure 2019Meris JugadorÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Pulp Volume Estimation Using CBCT-an in Vitro Pilot Study On Extracted Monoradicular TeethDocument7 paginiPulp Volume Estimation Using CBCT-an in Vitro Pilot Study On Extracted Monoradicular TeethMeris JugadorÎncă nu există evaluări
- Diffusion-Weighted Imaging in Acute Stroke - A Tool of Uncertain Value?Document10 paginiDiffusion-Weighted Imaging in Acute Stroke - A Tool of Uncertain Value?Meris JugadorÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Bateman2017Document6 paginiBateman2017Meris JugadorÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Diffusion-Weighted Magnetic Resonance ImagingDocument8 paginiDiffusion-Weighted Magnetic Resonance ImagingMeris JugadorÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- KumarDocument5 paginiKumarMeris JugadorÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Cjy 066Document9 paginiCjy 066Meris JugadorÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Role of CBCT in The Evaluation of Periodontal DiseasesDocument5 paginiThe Role of CBCT in The Evaluation of Periodontal DiseasesMeris JugadorÎncă nu există evaluări
- Cone-Beam Computed Tomography and Its Applications in DentistryDocument4 paginiCone-Beam Computed Tomography and Its Applications in DentistryMeris JugadorÎncă nu există evaluări
- Cone Beamed Computerized Dental Tomography in DentistryDocument5 paginiCone Beamed Computerized Dental Tomography in DentistryMeris JugadorÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Elif KarijesDocument9 paginiElif KarijesMeris JugadorÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Role of CBCT in Dental Caries Detection A Systematic ReviewDocument15 paginiRole of CBCT in Dental Caries Detection A Systematic ReviewMeris JugadorÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Prevalence of Apical Periodontitis Detected in Cone Beam CT Images of A Brazilian SubpopulationDocument6 paginiPrevalence of Apical Periodontitis Detected in Cone Beam CT Images of A Brazilian SubpopulationMeris JugadorÎncă nu există evaluări
- Zhang Age Estimation Using Pulpenamel Volume Ratio of ImpactedDocument9 paginiZhang Age Estimation Using Pulpenamel Volume Ratio of ImpactedMeris JugadorÎncă nu există evaluări
- Medical Hypotheses: D. Maret, O.A. Peters, F. Dedouit, N. Telmon, M. SixouDocument3 paginiMedical Hypotheses: D. Maret, O.A. Peters, F. Dedouit, N. Telmon, M. SixouMeris JugadorÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Dentistry Journal: Cone Beam Computed Tomography in Oral and Maxillofacial Surgery: An Evidence-Based ReviewDocument23 paginiDentistry Journal: Cone Beam Computed Tomography in Oral and Maxillofacial Surgery: An Evidence-Based ReviewMeris JugadorÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Age Estimation of Adults From Dental RadDocument11 paginiAge Estimation of Adults From Dental RadMeris JugadorÎncă nu există evaluări
- How To Estimate Dental Age in Paleodontology?: - Vedran Šebečić (1), Andrea Hoch (2), Maja Sabalić (2)Document6 paginiHow To Estimate Dental Age in Paleodontology?: - Vedran Šebečić (1), Andrea Hoch (2), Maja Sabalić (2)Meris JugadorÎncă nu există evaluări
- Gfa Ealth Are Ihe Integration Statement: Document No. 001549 Revision: 2 Nodeid Livelink: 57497642Document4 paginiGfa Ealth Are Ihe Integration Statement: Document No. 001549 Revision: 2 Nodeid Livelink: 57497642Meris JugadorÎncă nu există evaluări
- Role of Radiology in Forensic Dentistry PDFDocument3 paginiRole of Radiology in Forensic Dentistry PDFMeris JugadorÎncă nu există evaluări
- Age Estimation by Pulp Tooth Area Ratio in Anterior Teeth Using Cone-Beam Computed Tomography Comparison of Four TeethDocument8 paginiAge Estimation by Pulp Tooth Area Ratio in Anterior Teeth Using Cone-Beam Computed Tomography Comparison of Four TeethMeris JugadorÎncă nu există evaluări
- 3 Star2010Document6 pagini3 Star2010Meris JugadorÎncă nu există evaluări
- Cone Beam Computed Tomography Imaging of Dentoalveolar and Mandibular FracturesDocument8 paginiCone Beam Computed Tomography Imaging of Dentoalveolar and Mandibular FracturesMeris JugadorÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Age Estimation Using Pulp Tooth Volume Ratio by Cone Beam Computed TomographDocument6 paginiAge Estimation Using Pulp Tooth Volume Ratio by Cone Beam Computed TomographMeris JugadorÎncă nu există evaluări
- A New Age Estimation Procedure Based On The 3D CBCT Study of Thepulp Cavity and Hard Tissues of The Teeth For Forensic PurposesDocument3 paginiA New Age Estimation Procedure Based On The 3D CBCT Study of Thepulp Cavity and Hard Tissues of The Teeth For Forensic PurposesMeris JugadorÎncă nu există evaluări
- Class 11 Biology Notes Chapter 2 Studyguide360Document10 paginiClass 11 Biology Notes Chapter 2 Studyguide360AÎncă nu există evaluări
- Practical Research 2 - Chapter 1Document30 paginiPractical Research 2 - Chapter 1Luis ConcepcionÎncă nu există evaluări
- GRP 15 Property Law Final DDocument15 paginiGRP 15 Property Law Final DBruno OsananÎncă nu există evaluări
- Entrep 1st PerioDocument5 paginiEntrep 1st PerioMargarette FajardoÎncă nu există evaluări
- Economic and Product Design Considerations in MachiningDocument29 paginiEconomic and Product Design Considerations in Machininghashir siddiquiÎncă nu există evaluări
- Polevoque 3Document46 paginiPolevoque 3api-657593213Încă nu există evaluări
- Gremath Set8-1Document48 paginiGremath Set8-1uzairmetallurgistÎncă nu există evaluări
- MVVNL RGGVY Approved Vendor List: S.NO. Name of Material Vendor Name AddressDocument10 paginiMVVNL RGGVY Approved Vendor List: S.NO. Name of Material Vendor Name AddressELMEF LaboratoryÎncă nu există evaluări
- Assignment On How To Increase Own Brand Mantras: Submition Date: January 29,2021Document5 paginiAssignment On How To Increase Own Brand Mantras: Submition Date: January 29,2021Ferari DroboÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Frugal Innovation in Developed Markets - Adaption o - 2020 - Journal of InnovatiDocument9 paginiFrugal Innovation in Developed Markets - Adaption o - 2020 - Journal of InnovatiGisselle RomeroÎncă nu există evaluări
- Social Legislation Cases On Kasambahay LawDocument12 paginiSocial Legislation Cases On Kasambahay LawLiee Raine100% (1)
- General Request Form Graduate School, Chulalongkorn University (Only Use For Educational and Research Scholarship, Graduate School)Document2 paginiGeneral Request Form Graduate School, Chulalongkorn University (Only Use For Educational and Research Scholarship, Graduate School)Kyaw Zin PhyoÎncă nu există evaluări
- Preface: How To Use This BookDocument1 paginăPreface: How To Use This BookCarlos SaavedraÎncă nu există evaluări
- Stock Control Management SyestemDocument12 paginiStock Control Management SyestemJohn YohansÎncă nu există evaluări
- (2010) Formulaic Language and Second Language Speech Fluency - Background, Evidence and Classroom Applications-Continuum (2010)Document249 pagini(2010) Formulaic Language and Second Language Speech Fluency - Background, Evidence and Classroom Applications-Continuum (2010)Như Đặng QuếÎncă nu există evaluări
- Grade12 Rigel Group4 Assesing The Solid Waste Management Off Small Foos Store in Gingoog CityDocument31 paginiGrade12 Rigel Group4 Assesing The Solid Waste Management Off Small Foos Store in Gingoog CityMa. Joan ApolinarÎncă nu există evaluări
- 1404 1284 PDFDocument150 pagini1404 1284 PDFJohannRoaÎncă nu există evaluări
- Trading SecretsDocument99 paginiTrading SecretsGary100% (3)
- 9 - Report & NarrativeDocument1 pagină9 - Report & NarrativeTri WahyuningsihÎncă nu există evaluări
- The Basics of Effective Interpersonal Communication: by Sushila BahlDocument48 paginiThe Basics of Effective Interpersonal Communication: by Sushila BahlDevesh KhannaÎncă nu există evaluări
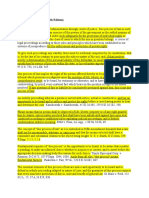
- Due Process of LawDocument2 paginiDue Process of Lawjoe100% (4)
- LESSON PLAN IN wRITING A REPORTDocument2 paginiLESSON PLAN IN wRITING A REPORTMarkaton Dihagnos100% (4)
- 2016 Biology CheckpointDocument14 pagini2016 Biology CheckpointNicholas Leong100% (1)
- Aficionado PERDocument19 paginiAficionado PERMaecaella LlorenteÎncă nu există evaluări
- Disruptive Strategy Final Paper Company ProfilesDocument2 paginiDisruptive Strategy Final Paper Company ProfilesHumberto Jose Arias BarrosÎncă nu există evaluări
- CWTS Narrative ReportDocument10 paginiCWTS Narrative ReportJa Rich100% (1)
- FSU7533 Digital Marketing & Social Media Career Advancement Certification (Including Voucher) ETPDocument2 paginiFSU7533 Digital Marketing & Social Media Career Advancement Certification (Including Voucher) ETPcÎncă nu există evaluări
- DHS/ICE (ICEPIC) Information Sharing Status: Enforcement Systems BranchDocument22 paginiDHS/ICE (ICEPIC) Information Sharing Status: Enforcement Systems BranchImpello_TyrannisÎncă nu există evaluări
- Part DDocument6 paginiPart DKaranja KinyanjuiÎncă nu există evaluări
- IGCSE-Revision-Booklet-Part-1-2018-2019 - (New-Spec)Document69 paginiIGCSE-Revision-Booklet-Part-1-2018-2019 - (New-Spec)MaryamÎncă nu există evaluări