S-ar putea să vă placă și
- Spinal Cord ND Spinal NervesDocument67 paginiSpinal Cord ND Spinal NervesfrizkapfÎncă nu există evaluări
- Cervical Disc 1Document68 paginiCervical Disc 1Nestor BalboaÎncă nu există evaluări
- Anotomy of PNS Irfan AliiDocument51 paginiAnotomy of PNS Irfan AliiAzeem Ali ShahÎncă nu există evaluări
- Structure of A Peripheral NerveDocument12 paginiStructure of A Peripheral NerveFides AdivisoÎncă nu există evaluări
- Anatomical LevelsDocument1 paginăAnatomical LevelspiemaningatÎncă nu există evaluări
- Anatomy Systema Nervosum Periphicum Et Autonomicum: Dr. Dodik NursantoDocument54 paginiAnatomy Systema Nervosum Periphicum Et Autonomicum: Dr. Dodik NursantoDhiastikaÎncă nu există evaluări
- Mri Spine by DR ShamolDocument309 paginiMri Spine by DR Shamolالقارئ محمد سيد عباس mohamed sayed abassÎncă nu există evaluări
- Lab 5 PNS & Spinal Cord AnswersDocument12 paginiLab 5 PNS & Spinal Cord AnswersCemre KuzeyÎncă nu există evaluări
- Back and Spinal Cord Study Guide: 2.1 Topographic Anatomy Study AimsDocument1 paginăBack and Spinal Cord Study Guide: 2.1 Topographic Anatomy Study AimsMihaelaÎncă nu există evaluări
- Brachial Plexus Block: "Dr. Sami Ur Rehman" House OfficerDocument65 paginiBrachial Plexus Block: "Dr. Sami Ur Rehman" House OfficerSami Ur RehmanÎncă nu există evaluări
- CH01 Sample PDFDocument32 paginiCH01 Sample PDFDilah RahmaÎncă nu există evaluări
- Description: SKELETAL SYSTEM-Axial SkeletonDocument18 paginiDescription: SKELETAL SYSTEM-Axial SkeletonJessica PalacioÎncă nu există evaluări
- EAU Pocket On Neuro Urology 2022Document13 paginiEAU Pocket On Neuro Urology 2022Dane QhÎncă nu există evaluări
- MRC Anatomy - Kadakia Final 2019Document247 paginiMRC Anatomy - Kadakia Final 20192qmdjr2qhkÎncă nu există evaluări
- Dermatomes+Myotomes Lower Limb Lecture SlidesDocument13 paginiDermatomes+Myotomes Lower Limb Lecture SlidesAnelisiwe DlaminiÎncă nu există evaluări
- 00 Neuro Cheat SheetDocument2 pagini00 Neuro Cheat SheetFranz LibreÎncă nu există evaluări
- Dr. AnanyaDocument55 paginiDr. AnanyatarawifaÎncă nu există evaluări
- Sci Additional NotesDocument16 paginiSci Additional NotesdescalzotahÎncă nu există evaluări
- Anatomy of Brachial Plexus: DR - Sadiq Wadood Siddiqui JR3 Department of AnatomyDocument53 paginiAnatomy of Brachial Plexus: DR - Sadiq Wadood Siddiqui JR3 Department of AnatomySadiq Wadood SiddiquiÎncă nu există evaluări
- Limbs 1b - Overview of Anatomy of Upper and Lower LimbsDocument5 paginiLimbs 1b - Overview of Anatomy of Upper and Lower LimbsTarmizi Md NorÎncă nu există evaluări
- Le Plexus BrachialDocument1 paginăLe Plexus BrachialCarl-Eric TanoéÎncă nu există evaluări
- Upper Limb MusclesDocument1 paginăUpper Limb MusclesVimala ColacoÎncă nu există evaluări
- Chapter 4 Sensory and Motor Pathways 2014 Clinical NeuroscienceDocument11 paginiChapter 4 Sensory and Motor Pathways 2014 Clinical NeuroscienceMarta Casals CollÎncă nu există evaluări
- Brachial PlexusDocument72 paginiBrachial PlexusmathivannaninthujanÎncă nu există evaluări
- UPPER LIMB - 6 Spinal Cord Segments, Dermatomes and Myotomes of The Upper LimbDocument3 paginiUPPER LIMB - 6 Spinal Cord Segments, Dermatomes and Myotomes of The Upper LimbAbbas AliÎncă nu există evaluări
- Brachial PlexusDocument5 paginiBrachial PlexusRajveerÎncă nu există evaluări
- Dr. Rohmania - Hernia Nukleus PulposusDocument30 paginiDr. Rohmania - Hernia Nukleus PulposusAnonymous FfZm5kOkYFÎncă nu există evaluări
- NIOM Anestesi (Autosaved) - 1Document58 paginiNIOM Anestesi (Autosaved) - 1andriruslyÎncă nu există evaluări
- How To Draw The Brachial PlexusDocument16 paginiHow To Draw The Brachial PlexusHÎncă nu există evaluări
- Pages From (Susan O'Sullivan, Raymond Siegelman) National PhyDocument1 paginăPages From (Susan O'Sullivan, Raymond Siegelman) National Phydrng48Încă nu există evaluări
- Muscle Origins, Insertions, Actions, and InterventionsDocument15 paginiMuscle Origins, Insertions, Actions, and InterventionsJoseph Kachelman100% (3)
- Muscles of The Superficial BackDocument3 paginiMuscles of The Superficial BackMargaux Chang NuñezÎncă nu există evaluări
- NETTER DermatomDocument1 paginăNETTER Dermatomngwinda90100% (1)
- Back MusclesDocument1 paginăBack MuscleslrostomeÎncă nu există evaluări
- The Brachial Plexus - Sections - Branches - TeachMeAnatomyDocument10 paginiThe Brachial Plexus - Sections - Branches - TeachMeAnatomymohit kumarÎncă nu există evaluări
- The Brain and Nerves: I I I I I I I I I I IDocument1 paginăThe Brain and Nerves: I I I I I I I I I I ISALIM BOUAIDÎncă nu există evaluări
- Branch of Brachialis PlexusDocument2 paginiBranch of Brachialis PlexusGrace GozaliÎncă nu există evaluări
- Key To Illustration: MUSCULAR SYSTEM-Skeletal MusclesDocument14 paginiKey To Illustration: MUSCULAR SYSTEM-Skeletal MusclesJessica PalacioÎncă nu există evaluări
- Brachial PlexusDocument4 paginiBrachial PlexussaluniasÎncă nu există evaluări
- Anatomy Supertable With Pics PDFDocument39 paginiAnatomy Supertable With Pics PDFCla NuvalÎncă nu există evaluări
- Vertebral Column: Nicole M. Reeves, Ph.D. Department of AnatomyDocument58 paginiVertebral Column: Nicole M. Reeves, Ph.D. Department of Anatomykrishna gÎncă nu există evaluări
- Lumbosacral PlexusDocument3 paginiLumbosacral Plexusgehaoi4Încă nu există evaluări
- Anatómia ÖsszefoglalóDocument4 paginiAnatómia ÖsszefoglalóvyolaÎncă nu există evaluări
- MSKDocument7 paginiMSKKY KimberlyÎncă nu există evaluări
- Ficha OsteowareDocument2 paginiFicha OsteowarearturosaezÎncă nu există evaluări
- Isncsci Worksheet 2015 Web PDFDocument2 paginiIsncsci Worksheet 2015 Web PDFDavideÎncă nu există evaluări
- Dr. Syed Irfan Raza ArifDocument27 paginiDr. Syed Irfan Raza ArifSyed Irfan ArifÎncă nu există evaluări
- Nerve Roots and Brancial PlexusDocument1 paginăNerve Roots and Brancial Plexuscyc9182Încă nu există evaluări
- And Physiology: The Human AnatomyDocument14 paginiAnd Physiology: The Human AnatomySakshi SharmaÎncă nu există evaluări
- 5 Orbit For Dental Students 2Document18 pagini5 Orbit For Dental Students 2Mohamad TallÎncă nu există evaluări
- MMT All MOVEMENTSDocument3 paginiMMT All MOVEMENTSesha NadeemÎncă nu există evaluări
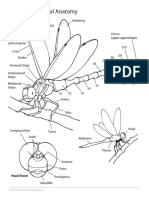
- Dragonfly External AnatomyDocument1 paginăDragonfly External AnatomyShizzy HeiwajimaÎncă nu există evaluări
- Chapter 1 - Overview of The Nervous System - 2014 - Clinical NeuroscienceDocument17 paginiChapter 1 - Overview of The Nervous System - 2014 - Clinical NeuroscienceMarta Casals CollÎncă nu există evaluări
- Right Totals (Maximum)Document6 paginiRight Totals (Maximum)kaychi zÎncă nu există evaluări
- Ilovepdf Merged MergedDocument11 paginiIlovepdf Merged MergedBbvcbÎncă nu există evaluări
- Table of Back Muscles RWDocument3 paginiTable of Back Muscles RWFrank Zhang100% (1)
- UntitledDocument59 paginiUntitledNidhish K ShettigarÎncă nu există evaluări
- Clavicular Head:: RD THDocument3 paginiClavicular Head:: RD THSam PadreÎncă nu există evaluări
- Patient Diagnosis Sheet PDFDocument1 paginăPatient Diagnosis Sheet PDFNaresh Muttavarapu100% (1)
- 7985 - Jadwal GIS 1920Document12 pagini7985 - Jadwal GIS 1920amelia rahayuÎncă nu există evaluări
- BCHDJKDocument17 paginiBCHDJKamelia rahayuÎncă nu există evaluări
- Jadwal Ujian Remedial Alih Tahun TAHUN AKADEMIK 2018 - 2019Document6 paginiJadwal Ujian Remedial Alih Tahun TAHUN AKADEMIK 2018 - 2019amelia rahayuÎncă nu există evaluări
- Laboratory Activity PhysiologyDocument10 paginiLaboratory Activity Physiologyamelia rahayuÎncă nu există evaluări
- Syllabus Laboratory Anatomy Gastrointestinal System: A SequenceDocument17 paginiSyllabus Laboratory Anatomy Gastrointestinal System: A Sequenceamelia rahayuÎncă nu există evaluări
- 9755 - IV Insertion TA 20192020 - WMDocument2 pagini9755 - IV Insertion TA 20192020 - WMamelia rahayuÎncă nu există evaluări
- FFF WPS OfficeDocument1 paginăFFF WPS Officeamelia rahayuÎncă nu există evaluări
- Intra Venous Insertion (Dr. DeddyDocument2 paginiIntra Venous Insertion (Dr. Deddyamelia rahayuÎncă nu există evaluări
- JhghiDocument7 paginiJhghiamelia rahayuÎncă nu există evaluări
- 7985 - Jadwal GIS 1920Document12 pagini7985 - Jadwal GIS 1920amelia rahayuÎncă nu există evaluări
- Laboratory Activity Physiology: Biomedical Laboratory, Faculty of Medicine, Unisba, Jl. Tamansari No.22 Bandung 40116Document4 paginiLaboratory Activity Physiology: Biomedical Laboratory, Faculty of Medicine, Unisba, Jl. Tamansari No.22 Bandung 40116amelia rahayuÎncă nu există evaluări
- (Letter Paper) Who Are You-WPS OfficeDocument1 pagină(Letter Paper) Who Are You-WPS Officeamelia rahayuÎncă nu există evaluări
- BHHJJ WPS OfficeDocument1 paginăBHHJJ WPS Officeamelia rahayuÎncă nu există evaluări
- KKLL WPS OfficeDocument1 paginăKKLL WPS Officeamelia rahayuÎncă nu există evaluări
- Superjunior WPS OfficeDocument1 paginăSuperjunior WPS Officeamelia rahayuÎncă nu există evaluări
- Hjnangzhhzhhzh WPS OfficeDocument1 paginăHjnangzhhzhhzh WPS Officeamelia rahayuÎncă nu există evaluări
- RGRDWD WPS OfficeDocument1 paginăRGRDWD WPS Officeamelia rahayuÎncă nu există evaluări
- Amajshb WPS OfficeDocument1 paginăAmajshb WPS Officeamelia rahayuÎncă nu există evaluări
- Apaan WPS OfficeDocument1 paginăApaan WPS Officeamelia rahayuÎncă nu există evaluări
- Superjunior WPS OfficeDocument1 paginăSuperjunior WPS Officeamelia rahayuÎncă nu există evaluări
- Intervertebral Disc Prolapse (Ivdp)Document42 paginiIntervertebral Disc Prolapse (Ivdp)salman h100% (3)
- Sacralization and Herniated Nucleus Pulposus An Association Study 2165 7939 1000297Document7 paginiSacralization and Herniated Nucleus Pulposus An Association Study 2165 7939 1000297Delfia AkiharyÎncă nu există evaluări
- Movement Stability and Lumbopelvic PainDocument638 paginiMovement Stability and Lumbopelvic PainYbergb Fbyr100% (8)
- Script Back SafetyDocument11 paginiScript Back SafetyEsnedaÎncă nu există evaluări
- Human Anatomy 4th Edition Mckinley Test BankDocument43 paginiHuman Anatomy 4th Edition Mckinley Test Bankjillhenrysetcjnzrfp100% (35)
- Effects Prolonged Sitting On Passive Flex I On StiffnessDocument10 paginiEffects Prolonged Sitting On Passive Flex I On StiffnessCharlie HigginsÎncă nu există evaluări
- Herniated Nucleus PulposusDocument29 paginiHerniated Nucleus PulposusRussel JanoloÎncă nu există evaluări
- Disorders of BonesDocument3 paginiDisorders of BonesAnonymous 0pSLjJYÎncă nu există evaluări
- Skeleetal Muscular SystemDocument2 paginiSkeleetal Muscular SystemJ MÎncă nu există evaluări
- Herniated Nucleus Pulposus in Dr. Hasan Sadikin General Hospital Bandung IndonesiaDocument7 paginiHerniated Nucleus Pulposus in Dr. Hasan Sadikin General Hospital Bandung Indonesiawulan dwi yulistiaÎncă nu există evaluări
- IvdpDocument89 paginiIvdpFelix SabuÎncă nu există evaluări
- Spine: Junior Intern - Csu College of MedicineDocument22 paginiSpine: Junior Intern - Csu College of MedicineCris Soliven DucosÎncă nu există evaluări
- Jurnal HNPDocument2 paginiJurnal HNPfebriÎncă nu există evaluări
- Nursing Care of The Patient Undergoing Lumbar Spinal Fusion: ReviewsDocument10 paginiNursing Care of The Patient Undergoing Lumbar Spinal Fusion: ReviewsMuammar100% (1)
- Differential Diagnoses For Disc HerniationDocument11 paginiDifferential Diagnoses For Disc HerniationZulvina FaozanudinÎncă nu există evaluări
- Medicine: Full-Endoscopic Discectomy Via The Interlaminar Approach For Disc Herniation at L4-L5 and L5-S1Document7 paginiMedicine: Full-Endoscopic Discectomy Via The Interlaminar Approach For Disc Herniation at L4-L5 and L5-S1Bell SwanÎncă nu există evaluări
- Back Pain How To Get Rid of It Permanently-1Document196 paginiBack Pain How To Get Rid of It Permanently-1alvishehzad9Încă nu există evaluări
- Percutaneous Disc Decompression in The Management of Chronic Low Back PainDocument7 paginiPercutaneous Disc Decompression in The Management of Chronic Low Back PainAlexandre Mio PosÎncă nu există evaluări
- SciticaDocument113 paginiSciticaBAKSON HMC DEGREESÎncă nu există evaluări
- Degenerative Disc Disease - Adrienne Ingalls PDFDocument34 paginiDegenerative Disc Disease - Adrienne Ingalls PDFVenkatesanSelvarajan100% (1)
- AnaphyDocument6 paginiAnaphyrhona esteibarÎncă nu există evaluări
- Summary Highlights of Yoga Secrets For Extraordinary Health and Long Life by Frank Rudolph YoungDocument62 paginiSummary Highlights of Yoga Secrets For Extraordinary Health and Long Life by Frank Rudolph Youngfmntime100% (7)
- Pilates For HerniationDocument10 paginiPilates For HerniationClaudia Liqui Politi100% (1)
- Lumbar SpineDocument43 paginiLumbar SpineVidhushi Vedhara100% (1)
- Anatomy of Vertebral ColumnDocument59 paginiAnatomy of Vertebral ColumnRivan DwiutomoÎncă nu există evaluări
- Ge15 - Manual Handling Awareness: Safe Moving and Handling of Loads December 2014Document63 paginiGe15 - Manual Handling Awareness: Safe Moving and Handling of Loads December 2014Samo BenÎncă nu există evaluări
- Gore-Endoworld 41224500 PDFDocument32 paginiGore-Endoworld 41224500 PDFKaustubh Keskar100% (1)
- PM&R in Degenearative Joint DiseaseDocument66 paginiPM&R in Degenearative Joint DiseaseLorenz SmallÎncă nu există evaluări
- Pott's DiseaseDocument11 paginiPott's DiseaseNicole Anne ValerioÎncă nu există evaluări
- Cervical Disc Disease and Spondylosis: Rabia Qureshi, Jason A. Horowitz, Hamid HassanzadehDocument7 paginiCervical Disc Disease and Spondylosis: Rabia Qureshi, Jason A. Horowitz, Hamid HassanzadehMasithaÎncă nu există evaluări