S-ar putea să vă placă și
- The neurologists: A history of a medical specialty in modern Britain, c.1789–2000De la EverandThe neurologists: A history of a medical specialty in modern Britain, c.1789–2000Încă nu există evaluări
- Great Feuds in Medicine: Ten of the Liveliest Disputes EverDe la EverandGreat Feuds in Medicine: Ten of the Liveliest Disputes EverEvaluare: 3.5 din 5 stele3.5/5 (19)
- Neuroendocrinology: Volume IDe la EverandNeuroendocrinology: Volume ILuciano MartiniÎncă nu există evaluări
- A Matter of Life and Death: Inside the Hidden World of the PathologistDe la EverandA Matter of Life and Death: Inside the Hidden World of the PathologistEvaluare: 4 din 5 stele4/5 (2)
- The New Neurotology: A Comprehensive Clinical GuideDe la EverandThe New Neurotology: A Comprehensive Clinical GuideÎncă nu există evaluări
- Hazards of the Job: From Industrial Disease to Environmental Health ScienceDe la EverandHazards of the Job: From Industrial Disease to Environmental Health ScienceÎncă nu există evaluări
- Doctors in Denial: The Forgotten Women in the 'Unfortunate Experiment'De la EverandDoctors in Denial: The Forgotten Women in the 'Unfortunate Experiment'Evaluare: 5 din 5 stele5/5 (1)
- Behavior and Cognitive Therapy Today: Essays in Honor of Hans J. Eysenck: Essays in Honour of Hans J. EysenckDe la EverandBehavior and Cognitive Therapy Today: Essays in Honor of Hans J. Eysenck: Essays in Honour of Hans J. EysenckE. SanavioÎncă nu există evaluări
- Laryngoscopy - Its Past and Future: Canadian Anaesthetists? Society Journal June 2004Document6 paginiLaryngoscopy - Its Past and Future: Canadian Anaesthetists? Society Journal June 2004razihaikalÎncă nu există evaluări
- Boyer Lectures 2014: The Promise of Science - A Vision of HopeDe la EverandBoyer Lectures 2014: The Promise of Science - A Vision of HopeÎncă nu există evaluări
- Extraordinary Healing: How the Discoveries of Mirko Beljanski, the World's First Green Molecular Biologist, Can Protect andDe la EverandExtraordinary Healing: How the Discoveries of Mirko Beljanski, the World's First Green Molecular Biologist, Can Protect andÎncă nu există evaluări
- A Physician's Handbook on Orthomolecular MedicineDe la EverandA Physician's Handbook on Orthomolecular MedicineEvaluare: 2.5 din 5 stele2.5/5 (2)
- The Virus and the Vaccine: The True Story of a Cancer-Causing Monkey Virus, Contaminated Polio Vaccine, and the Millions of Americans ExposedDe la EverandThe Virus and the Vaccine: The True Story of a Cancer-Causing Monkey Virus, Contaminated Polio Vaccine, and the Millions of Americans ExposedEvaluare: 3.5 din 5 stele3.5/5 (6)
- PetrovicDocument2 paginiPetrovicGabriela LouÎncă nu există evaluări
- The Clinical and Scientific Basis of Myalgic Encephalomyelitis/ Chronic Fatigue Syndrome Byron M. Hyde, M.D.Document753 paginiThe Clinical and Scientific Basis of Myalgic Encephalomyelitis/ Chronic Fatigue Syndrome Byron M. Hyde, M.D.Gènia100% (2)
- Summary of The Song of the Cell By Siddhartha Mukherjee: An Exploration of Medicine and the New HumanDe la EverandSummary of The Song of the Cell By Siddhartha Mukherjee: An Exploration of Medicine and the New HumanEvaluare: 5 din 5 stele5/5 (1)
- NeuroTribes: The Legacy of Autism and the Future of Neurodiversity by Steve Silberman | Key Takeaways, Analysis & ReviewDe la EverandNeuroTribes: The Legacy of Autism and the Future of Neurodiversity by Steve Silberman | Key Takeaways, Analysis & ReviewEvaluare: 4.5 din 5 stele4.5/5 (215)
- In Memoriam: Carl C. Pfeiffer, - ., PH.D., - .: B A M DDocument2 paginiIn Memoriam: Carl C. Pfeiffer, - ., PH.D., - .: B A M DSchwab RealHumanÎncă nu există evaluări
- Dr. Folkman's War: Angiogenesis and the Struggle to Defeat CancerDe la EverandDr. Folkman's War: Angiogenesis and the Struggle to Defeat CancerEvaluare: 4.5 din 5 stele4.5/5 (8)
- Nervous Systems: Brain Science in the Early Cold WarDe la EverandNervous Systems: Brain Science in the Early Cold WarÎncă nu există evaluări
- Famous Discoveries by Medical StudentsansDocument8 paginiFamous Discoveries by Medical StudentsansJoao FonsecaÎncă nu există evaluări
- SDFGDocument9 paginiSDFGapi-257859692Încă nu există evaluări
- Tending Adam's Garden: Evolving the Cognitive Immune SelfDe la EverandTending Adam's Garden: Evolving the Cognitive Immune SelfÎncă nu există evaluări
- John Parks Trowbridge M. D., FACAM: "Inquiring Minds Want To Know "Document13 paginiJohn Parks Trowbridge M. D., FACAM: "Inquiring Minds Want To Know "AlexÎncă nu există evaluări
- Epigenetics: The Death of the Genetic Theory of Disease TransmissionDe la EverandEpigenetics: The Death of the Genetic Theory of Disease TransmissionEvaluare: 3.5 din 5 stele3.5/5 (7)
- Headington Hill Hall the forgotten years 1939 to 1958De la EverandHeadington Hill Hall the forgotten years 1939 to 1958Încă nu există evaluări
- Dale's an Introduction to Social BiologyDe la EverandDale's an Introduction to Social BiologySusan DaleÎncă nu există evaluări
- Boundaries of Evolution: What Would Darwin Think Now About Dna, the Big Bang, and Finite Time?De la EverandBoundaries of Evolution: What Would Darwin Think Now About Dna, the Big Bang, and Finite Time?Încă nu există evaluări
- Stem Cell Dialogues: A Philosophical and Scientific Inquiry Into Medical FrontiersDe la EverandStem Cell Dialogues: A Philosophical and Scientific Inquiry Into Medical FrontiersÎncă nu există evaluări
- Hepatitis B: The Hunt for a Killer VirusDe la EverandHepatitis B: The Hunt for a Killer VirusEvaluare: 2 din 5 stele2/5 (2)
- Scientists Who Worked On PhysiologyDocument22 paginiScientists Who Worked On Physiologyhermyohknee212Încă nu există evaluări
- Articolo Su Dale - Todman (2007) - Henry Dale and The Discovery of Chemical Synaptic TransmissionDocument3 paginiArticolo Su Dale - Todman (2007) - Henry Dale and The Discovery of Chemical Synaptic TransmissionFrancesca CostaÎncă nu există evaluări
- Bernard Jensen - Iridology PDFDocument610 paginiBernard Jensen - Iridology PDFAurora Miko100% (7)
- Cuban Blindness: Diary of a Mysterious Epidemic NeuropathyDe la EverandCuban Blindness: Diary of a Mysterious Epidemic NeuropathyÎncă nu există evaluări
- Orthopaedic NeurologyDocument134 paginiOrthopaedic NeurologyRaymond Parung100% (1)
- Of Vets, Viruses and Vaccines: The Story of the Animal Health Research Laboratory, ParkvilleDe la EverandOf Vets, Viruses and Vaccines: The Story of the Animal Health Research Laboratory, ParkvilleÎncă nu există evaluări
- Little Masterpieces of Science: Health and HealingDe la EverandLittle Masterpieces of Science: Health and HealingÎncă nu există evaluări
- Neurosyphilis: Modern Systematic Diagnosis and Treatment Presented in One Hundred and Thirty-Seven Case HistoriesDe la EverandNeurosyphilis: Modern Systematic Diagnosis and Treatment Presented in One Hundred and Thirty-Seven Case HistoriesÎncă nu există evaluări
- THE TROUBLE WITH DOCTORS: FRAUD AND DECEIT IN MEDICINE: FRAUD AND DECEIT IN MEDICINEDe la EverandTHE TROUBLE WITH DOCTORS: FRAUD AND DECEIT IN MEDICINE: FRAUD AND DECEIT IN MEDICINEÎncă nu există evaluări
- Science 100: Science, Technology and Society: Lesson 2: Nature of TechnologyDocument9 paginiScience 100: Science, Technology and Society: Lesson 2: Nature of Technology이시연Încă nu există evaluări
- Summary of The Immortal Life of Henrietta Lacks: by Rebecca Skloot - A Comprehensive SummaryDe la EverandSummary of The Immortal Life of Henrietta Lacks: by Rebecca Skloot - A Comprehensive SummaryÎncă nu există evaluări
- The Power of Stories in Pediatrics and Genetics: Commentary Open AccessDocument11 paginiThe Power of Stories in Pediatrics and Genetics: Commentary Open AccessShanna JocelynÎncă nu există evaluări
- Brain Function: Cortical Excitability and Steady Potentials; Relations of Basic Research to Space BiologyDe la EverandBrain Function: Cortical Excitability and Steady Potentials; Relations of Basic Research to Space BiologyÎncă nu există evaluări
- Early Victims of X-Rays: A Tribute and Current PerceptionDocument3 paginiEarly Victims of X-Rays: A Tribute and Current PerceptionFlávio Augusto SoaresÎncă nu există evaluări
- Parkinson S Disease and Related Disorders Part II PDFDocument570 paginiParkinson S Disease and Related Disorders Part II PDFskyclad_21Încă nu există evaluări
- The Spiral After-Effect: International Series of Monographs in Experimental Psychology, Volume 2De la EverandThe Spiral After-Effect: International Series of Monographs in Experimental Psychology, Volume 2Încă nu există evaluări
- Cell Biology Meets Rolfing: NewsfocusDocument2 paginiCell Biology Meets Rolfing: Newsfocusrcastello20Încă nu există evaluări
- Our Sense of Direction - Progress, Controversies and Challenges Kathleen E Cullen1 & Jeffrey S Taube2 (2017)Document9 paginiOur Sense of Direction - Progress, Controversies and Challenges Kathleen E Cullen1 & Jeffrey S Taube2 (2017)J WÎncă nu există evaluări
- MRI-Defined White Matter Microstructural Alteration Associated With Soccer Heading Is More Extensive in Women Than Men. Rubin 2018Document9 paginiMRI-Defined White Matter Microstructural Alteration Associated With Soccer Heading Is More Extensive in Women Than Men. Rubin 2018J WÎncă nu există evaluări
- Acute Unilateral Vestibulopathy Strupp & Magnusson (2015)Document17 paginiAcute Unilateral Vestibulopathy Strupp & Magnusson (2015)J WÎncă nu există evaluări
- 2014 - Perez-Fornos Et Al - Artificial Balance VOR RestorationDocument11 pagini2014 - Perez-Fornos Et Al - Artificial Balance VOR RestorationJ WÎncă nu există evaluări
- Perilymph FistulaDocument4 paginiPerilymph FistulavieeveeÎncă nu există evaluări
- Clinical Manual of OtolaryngologyDocument49 paginiClinical Manual of Otolaryngologygamecockusc1992100% (3)
- 6 Sound at WorkDocument17 pagini6 Sound at Workapi-200253170Încă nu există evaluări
- COCHLEADocument7 paginiCOCHLEALubna LiyakatÎncă nu există evaluări
- Special Senses NotesDocument3 paginiSpecial Senses NotesChelsa LeyritanaÎncă nu există evaluări
- Introduction To Psychology 10th Edition Plotnik Test Bank 1Document38 paginiIntroduction To Psychology 10th Edition Plotnik Test Bank 1norma100% (47)
- Vestibular NeuronitisDocument3 paginiVestibular NeuronitisAnish RajÎncă nu există evaluări
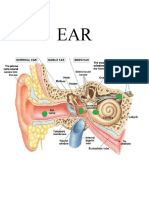
- Anatomy EarDocument20 paginiAnatomy EarRod HilalÎncă nu există evaluări
- Chapter 2: Articulatory, Auditory and Acoustic Phonetics. PhonologyDocument4 paginiChapter 2: Articulatory, Auditory and Acoustic Phonetics. PhonologycalluraÎncă nu există evaluări
- Ear Disorder Multiple Choice Questions-RationaleDocument5 paginiEar Disorder Multiple Choice Questions-Rationalemydewyboy83% (6)
- 2nd SUMMATIVE 2019 in Science 3Document1 pagină2nd SUMMATIVE 2019 in Science 3Nash PerezÎncă nu există evaluări
- Van 13Document5 paginiVan 13citra butar butarÎncă nu există evaluări
- Ears Lecture GuideDocument56 paginiEars Lecture GuidemajÎncă nu există evaluări
- Principles of Anatomy and Physiology: 14 EditionDocument62 paginiPrinciples of Anatomy and Physiology: 14 EditionWilliam C Chisha100% (1)
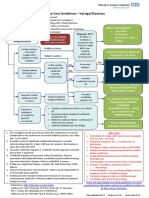
- Management of Vertigo - DR - Attiya Rahma SpsDocument59 paginiManagement of Vertigo - DR - Attiya Rahma SpsHenni Pus Vera100% (1)
- Auditory and Visual Pathways - A Mixed Course-Based Research Approach To Human PhysiologyDocument14 paginiAuditory and Visual Pathways - A Mixed Course-Based Research Approach To Human PhysiologyIncognito 000Încă nu există evaluări
- The Use of Laser Doppler Vibrometry Doppler Principle For Middle Ear Research and DiagnosisDocument8 paginiThe Use of Laser Doppler Vibrometry Doppler Principle For Middle Ear Research and DiagnosisHoria MocanuÎncă nu există evaluări
- Noise Reduction Rating (NRR) : Theresa Y. Schulz, PHD, Ltcol, Usaf (Ret.)Document18 paginiNoise Reduction Rating (NRR) : Theresa Y. Schulz, PHD, Ltcol, Usaf (Ret.)temterÎncă nu există evaluări
- Information ProcessingDocument51 paginiInformation ProcessingNurizni100% (1)
- Children With Hearing ImpairmentDocument10 paginiChildren With Hearing ImpairmentAfifah MiftahÎncă nu există evaluări
- Functional Cortical Areas of BrainDocument10 paginiFunctional Cortical Areas of BrainAdeel MasoodÎncă nu există evaluări
- Nadlif Muammar KH KhumainiDocument1 paginăNadlif Muammar KH KhumainiBoca PetualangÎncă nu există evaluări
- Otitis MediaDocument6 paginiOtitis Mediafrances1828Încă nu există evaluări
- Comprehensive Board Exam ENT PDFDocument644 paginiComprehensive Board Exam ENT PDFdrskbarla50% (2)
- ENT Vertigo FINAL v0.41Document1 paginăENT Vertigo FINAL v0.41Farmasi BhamadaÎncă nu există evaluări
- SensationDocument173 paginiSensationapi-261267976Încă nu există evaluări
- Acoustic - Stapedius - Reflexes PDFDocument6 paginiAcoustic - Stapedius - Reflexes PDFSOFTMERCURYÎncă nu există evaluări
- 6th Class General Science Chapter 2Document2 pagini6th Class General Science Chapter 2Shahid MahmoodÎncă nu există evaluări
- Acoustic NeuromaDocument6 paginiAcoustic NeuromayoghaÎncă nu există evaluări
- Perforated EardrumDocument5 paginiPerforated EardrumElvinÎncă nu există evaluări