S-ar putea să vă placă și
- Employment AgreementDocument8 paginiEmployment Agreementjohn100% (9)
- Unfree Masters by Matt StahlDocument42 paginiUnfree Masters by Matt StahlDuke University Press100% (1)
- Letter To The EditorDocument4 paginiLetter To The EditorMarnie TonsonÎncă nu există evaluări
- Manager Shadowing ChecklistDocument4 paginiManager Shadowing Checklistapi-370434100Încă nu există evaluări
- Ansi - Isa-75 08 01-2002Document18 paginiAnsi - Isa-75 08 01-2002jleonosÎncă nu există evaluări
- Drug Testing Laboratory LawsDocument77 paginiDrug Testing Laboratory LawsKrisyah Niqoule ValdezÎncă nu există evaluări
- Agrarian Law and Social Legislation NotesDocument26 paginiAgrarian Law and Social Legislation NotesSanson OrozcoÎncă nu există evaluări
- Barrister Magazine Issue 41Document21 paginiBarrister Magazine Issue 41kered1954Încă nu există evaluări
- Kaiser Permanente California Plans and Benefits Brochure KPIF 2011Document6 paginiKaiser Permanente California Plans and Benefits Brochure KPIF 2011DennisÎncă nu există evaluări
- 2010 UHC Medical Plan ComparisonDocument2 pagini2010 UHC Medical Plan Comparisonapi-20618861Încă nu există evaluări
- Core MVDocument1 paginăCore MVGowell SupportÎncă nu există evaluări
- First Help PlanDocument1 paginăFirst Help PlanIvan QuevedoÎncă nu există evaluări
- 2022 Steven Charles BAG - CODocument4 pagini2022 Steven Charles BAG - COAlejuanchis Kamacho GarciaÎncă nu există evaluări
- 2023 Talent BAAGDocument3 pagini2023 Talent BAAGThi HanÎncă nu există evaluări
- Benefit Highlights: AARP Medicare Advantage Choice (PPO)Document3 paginiBenefit Highlights: AARP Medicare Advantage Choice (PPO)EstherÎncă nu există evaluări
- Kaiser Permanente Compare Plans CA 2011 KPIFDocument1 paginăKaiser Permanente Compare Plans CA 2011 KPIFDennis AlexanderÎncă nu există evaluări
- Choice MVDocument1 paginăChoice MVGowell SupportÎncă nu există evaluări
- EmblemHealth Benefits 2019Document7 paginiEmblemHealth Benefits 2019Jorge Luis Rivera AgostoÎncă nu există evaluări
- Summary of 2022 Benefit Changes: MedicalDocument5 paginiSummary of 2022 Benefit Changes: MedicalChinnu SalimathÎncă nu există evaluări
- Pet Insurance ComparisonsDocument2 paginiPet Insurance ComparisonsHSVC50% (2)
- ProductsDocument3 paginiProductsYaseenÎncă nu există evaluări
- Harmonic ScalpelDocument2 paginiHarmonic ScalpelHerman HalimÎncă nu există evaluări
- M2A1 US Census Data SearchDocument6 paginiM2A1 US Census Data SearchragcajunÎncă nu există evaluări
- Summary of Benefits: Silver Trio Hmo 2300/70 OffexDocument12 paginiSummary of Benefits: Silver Trio Hmo 2300/70 OffexjaroopaitummaiÎncă nu există evaluări
- The Essential Plan Chart WnyDocument1 paginăThe Essential Plan Chart WnyJavier GramajoÎncă nu există evaluări
- Blueshield Gold Trio HMO 1500:35Document14 paginiBlueshield Gold Trio HMO 1500:35jaroopaitummaiÎncă nu există evaluări
- Benefit at A GlanceDocument2 paginiBenefit at A GlanceShiv ChauhanÎncă nu există evaluări
- Schedule of BenefitsDocument7 paginiSchedule of BenefitsMaddy CruzÎncă nu există evaluări
- AARP UHC 2024 Benefit Highlights LA 004P FocusDocument4 paginiAARP UHC 2024 Benefit Highlights LA 004P FocusAlaa ZaidÎncă nu există evaluări
- Book1 (Version 1)Document1 paginăBook1 (Version 1)agulabÎncă nu există evaluări
- Generic Open Enrollment KitDocument22 paginiGeneric Open Enrollment KitSteve BarrowsÎncă nu există evaluări
- Benefits Highlights 2018Document5 paginiBenefits Highlights 2018Marcus CosmeÎncă nu există evaluări
- Keystone HMO Gold Preferred 4080650Document11 paginiKeystone HMO Gold Preferred 4080650ANKIT SINGHÎncă nu există evaluări
- Medical Comparison Chart 2020Document3 paginiMedical Comparison Chart 2020hollingermikeÎncă nu există evaluări
- Young Adult BrochureDocument5 paginiYoung Adult BrochureahsanÎncă nu există evaluări
- Summary of Benefits: Bronze Trio Hmo 7000/70 OffexDocument12 paginiSummary of Benefits: Bronze Trio Hmo 7000/70 OffexjaroopaitummaiÎncă nu există evaluări
- Unitedhealthcare Dental Hmo Plan 2022 Summary of Benefits and CoverageDocument9 paginiUnitedhealthcare Dental Hmo Plan 2022 Summary of Benefits and CoverageAdam CliftonÎncă nu există evaluări
- ConvertDocument2 paginiConvertpham_thu_hangÎncă nu există evaluări
- Cardea Schedule of Benefits Effective Jan 1st 2021Document4 paginiCardea Schedule of Benefits Effective Jan 1st 2021Wayne GajadharÎncă nu există evaluări
- Women's Reproductive Health Free Clinic: Personnel ExpensesDocument2 paginiWomen's Reproductive Health Free Clinic: Personnel ExpensesHujale MaxamedÎncă nu există evaluări
- Photon Benefits 2022 (August)Document7 paginiPhoton Benefits 2022 (August)sojithesouljaÎncă nu există evaluări
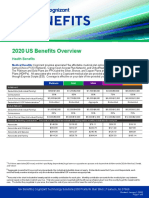
- 2020 US Benefits OverviewDocument5 pagini2020 US Benefits OverviewrdmÎncă nu există evaluări
- Silver EssentialDocument4 paginiSilver EssentialVasikaran PrabaharanÎncă nu există evaluări
- Special Care and Adultbasic: Comparison ChartDocument1 paginăSpecial Care and Adultbasic: Comparison ChartjhsmalankaÎncă nu există evaluări
- Group Project 1Document21 paginiGroup Project 1api-547174770Încă nu există evaluări
- Bronze HSA 5000Document4 paginiBronze HSA 5000Vasikaran PrabaharanÎncă nu există evaluări
- 2023 Open Enrollment Benefit Presenation - 11142022Document30 pagini2023 Open Enrollment Benefit Presenation - 11142022margreen5Încă nu există evaluări
- Plan ComparisonDocument4 paginiPlan Comparisontth79hj4dvÎncă nu există evaluări
- LTIM - USA Employees Benefits Overview - 2024Document20 paginiLTIM - USA Employees Benefits Overview - 2024Ramesh Kumar KÎncă nu există evaluări
- ViewyoursbcdocumentDocument12 paginiViewyoursbcdocumentapi-531507901Încă nu există evaluări
- 2017 Employee Benefit Highlights - Support StaffDocument8 pagini2017 Employee Benefit Highlights - Support StaffJohn AcardoÎncă nu există evaluări
- Your Total Rewards at Newyork-PresbyterianDocument20 paginiYour Total Rewards at Newyork-PresbyterianweiweiahÎncă nu există evaluări
- Aurora - Baseline Option 2019 SOBIDocument4 paginiAurora - Baseline Option 2019 SOBISean MurrayÎncă nu există evaluări
- KP - Plan Summary Medical - PPODocument3 paginiKP - Plan Summary Medical - PPOshanegbaker51Încă nu există evaluări
- Trinity Health 020 Traditional Ppo Plan 10202021Document10 paginiTrinity Health 020 Traditional Ppo Plan 10202021emily WÎncă nu există evaluări
- What You Pay in The PPO PlanDocument2 paginiWhat You Pay in The PPO Plannathan wongÎncă nu există evaluări
- Eb 2019 Oe Guideplussbc GenericDocument19 paginiEb 2019 Oe Guideplussbc GenericCybernaughtÎncă nu există evaluări
- Everyday Extras: Get The Same Amount Back Each Time You VisitDocument2 paginiEveryday Extras: Get The Same Amount Back Each Time You Visitfrank.wangÎncă nu există evaluări
- Plan ComparisonDocument2 paginiPlan ComparisonSahil JindalÎncă nu există evaluări
- Fhpv23apr231218j7r2 Veasna UkDocument6 paginiFhpv23apr231218j7r2 Veasna UkSela SinÎncă nu există evaluări
- Kaiser Permanente: Good Health Is No SecretDocument6 paginiKaiser Permanente: Good Health Is No SecretThomas Dominic CazneauÎncă nu există evaluări
- Plan Comparison Chart Seniorcare Hip AetnaDocument5 paginiPlan Comparison Chart Seniorcare Hip AetnaRamonita GarciaÎncă nu există evaluări
- 76962CT0010006-01 en USDocument98 pagini76962CT0010006-01 en USKathy ApergisÎncă nu există evaluări
- Cs Plus NYC Area Epo 2q 2009Document1 paginăCs Plus NYC Area Epo 2q 2009KristieÎncă nu există evaluări
- Protect What You Treasure Most: HealthDocument12 paginiProtect What You Treasure Most: HealthNelly HÎncă nu există evaluări
- Tricare Costs and Fees: TRICARE PRIME® COSTS (Jan. 1-Dec. 31) Tricare Select Costs (Jan. 1-Dec. 31)Document4 paginiTricare Costs and Fees: TRICARE PRIME® COSTS (Jan. 1-Dec. 31) Tricare Select Costs (Jan. 1-Dec. 31)FRANKLYN TRONCOÎncă nu există evaluări
- Brochure - EZCare (Nov 2022)Document11 paginiBrochure - EZCare (Nov 2022)Darren ChenÎncă nu există evaluări
- Ethics Chapter 5Document7 paginiEthics Chapter 5mine2515100% (1)
- RA Respiratory Davao Sept2019 PDFDocument5 paginiRA Respiratory Davao Sept2019 PDFPhilBoardResultsÎncă nu există evaluări
- Principle of Macroeconomics Bbek4203Document17 paginiPrinciple of Macroeconomics Bbek4203SHANU NAIR A/P SASEEDHAARAN studentÎncă nu există evaluări
- Kurita Ax 734pDocument2 paginiKurita Ax 734pSim Khoon AunÎncă nu există evaluări
- Federal Register / Vol. 71, No. 106 / Friday, June 2, 2006 / Rules and RegulationsDocument18 paginiFederal Register / Vol. 71, No. 106 / Friday, June 2, 2006 / Rules and RegulationsJustia.comÎncă nu există evaluări
- NLC Personnel Manual Vol II PDFDocument210 paginiNLC Personnel Manual Vol II PDFBharAth ReDdyÎncă nu există evaluări
- Strategic Frame Analysis & Policy Making: Where Does SFA Fit Into Our Strategic Plan?Document10 paginiStrategic Frame Analysis & Policy Making: Where Does SFA Fit Into Our Strategic Plan?Benedikt HorvatÎncă nu există evaluări
- FSDFSDFSDFSDFSDDocument4 paginiFSDFSDFSDFSDFSDylessinÎncă nu există evaluări
- Scheme 2023 and 2022 (Central Govt)Document77 paginiScheme 2023 and 2022 (Central Govt)Kartik SharmaÎncă nu există evaluări
- 2023.admin Law - Syllabus and Case List - Part 1Document2 pagini2023.admin Law - Syllabus and Case List - Part 1LoÎncă nu există evaluări
- TALAB Reflection PaperDocument2 paginiTALAB Reflection PaperCoralie LagamayoÎncă nu există evaluări
- Supporting Change in Assam Jan 19 UpdateDocument5 paginiSupporting Change in Assam Jan 19 UpdateSatyabrata NayakÎncă nu există evaluări
- Display Screen Equipment PolicyDocument2 paginiDisplay Screen Equipment PolicyRameeSahibaÎncă nu există evaluări
- Sample Solved Question Papers For Irda 25 Hours Agents Training Exam Foric-38Document13 paginiSample Solved Question Papers For Irda 25 Hours Agents Training Exam Foric-38SONÎncă nu există evaluări
- Ehr Recommendation ReportDocument8 paginiEhr Recommendation Reportapi-356200224Încă nu există evaluări
- Progressive D BQDocument7 paginiProgressive D BQryan3708Încă nu există evaluări
- CR2019-001522 2014-09sep-29 CASA - CASA Affidavit - Redacted - Court Appointed Special Advocate - 4 PagesDocument4 paginiCR2019-001522 2014-09sep-29 CASA - CASA Affidavit - Redacted - Court Appointed Special Advocate - 4 PagesmikekvolpeÎncă nu există evaluări
- Form Licence ConductorDocument3 paginiForm Licence ConductorBaljeet Singh100% (1)
- Cur 518 Organization Diveristy Planning PresentationDocument10 paginiCur 518 Organization Diveristy Planning Presentationapi-279315678Încă nu există evaluări
- Mtech0314 DavaoDocument3 paginiMtech0314 DavaoangelomercedeblogÎncă nu există evaluări
- Kansas RFP Evt0001028Document171 paginiKansas RFP Evt0001028infochghealthÎncă nu există evaluări
- 01 Gen Prov With GPP OverviewOct2019Document110 pagini01 Gen Prov With GPP OverviewOct2019Jay TeeÎncă nu există evaluări