S-ar putea să vă placă și
- Postgraduate Notes in OrthodonticsDocument257 paginiPostgraduate Notes in OrthodonticsSabrina Nitulescu100% (4)
- Management of Patients On Systemic Steroids - An Oral Surgery PerspectiveDocument7 paginiManagement of Patients On Systemic Steroids - An Oral Surgery PerspectiveMohammad Abdulmon’emÎncă nu există evaluări
- Oral Wound Healing: Cell Biology and Clinical ManagementDe la EverandOral Wound Healing: Cell Biology and Clinical ManagementHannu LarjavaÎncă nu există evaluări
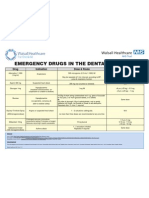
- Emergency Drugs Poster - Layout 1 in Dental PracticeDocument1 paginăEmergency Drugs Poster - Layout 1 in Dental PracticeFady AtefÎncă nu există evaluări
- NATIONAL DENTAL BOARDS (NDB) / PART I: Passbooks Study GuideDe la EverandNATIONAL DENTAL BOARDS (NDB) / PART I: Passbooks Study GuideEvaluare: 1 din 5 stele1/5 (1)
- Diagnosis and Treatment Planning For Partially Edentulous Patients11Document160 paginiDiagnosis and Treatment Planning For Partially Edentulous Patients11Rajsandeep Singh80% (5)
- Diagnosis and Treatment Planning For Partially Edentulous Patients11Document160 paginiDiagnosis and Treatment Planning For Partially Edentulous Patients11Rajsandeep Singh80% (5)
- 1885 2Document73 pagini1885 2JuhiJahan AmanullahÎncă nu există evaluări
- 11 Residual Ridge ResorptionDocument66 pagini11 Residual Ridge ResorptionSuman JainÎncă nu există evaluări
- Principles of Occlusion in Complete DentureDocument72 paginiPrinciples of Occlusion in Complete DentureDaniel AtiehÎncă nu există evaluări
- Pre Malignant LesionsDocument89 paginiPre Malignant LesionsmaheshopÎncă nu există evaluări
- TMJ AnatomiDocument53 paginiTMJ AnatomiNiTa DöéMy HarDianaÎncă nu există evaluări
- NUTRITION & Its Role in PeriodontologyDocument73 paginiNUTRITION & Its Role in Periodontologyshivi2014100% (1)
- Rationale For Periodontal TherapyDocument22 paginiRationale For Periodontal TherapyRajani GedelaÎncă nu există evaluări
- Avulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The ToothDocument39 paginiAvulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The Toothshailesh_shenoyÎncă nu există evaluări
- Stem CellDocument17 paginiStem Cellsonal agarwalÎncă nu există evaluări
- Try in AppointmentDocument91 paginiTry in Appointmentspu123Încă nu există evaluări
- Consent To Periodontal SurgeryDocument2 paginiConsent To Periodontal SurgeryJitender ReddyÎncă nu există evaluări
- Dental Ceramics: Hamna Nadeem Roll No. 30Document6 paginiDental Ceramics: Hamna Nadeem Roll No. 30sash34Încă nu există evaluări
- CLASSIC ARTICLE-Evaluation of The Factors Necessary To Develop Stability in Mandibular Dentures-Corwin R. WrightDocument10 paginiCLASSIC ARTICLE-Evaluation of The Factors Necessary To Develop Stability in Mandibular Dentures-Corwin R. WrightChander UdheyÎncă nu există evaluări
- Cysts of The Oral RegionDocument5 paginiCysts of The Oral RegionPaul Anthony Garcia ConcepcionÎncă nu există evaluări
- Medical Engineering & PhysicsDocument6 paginiMedical Engineering & PhysicsLuis Fernando Guayllas PomaÎncă nu există evaluări
- Osman, Pallagud - Periodontal Disease Rate NewDocument22 paginiOsman, Pallagud - Periodontal Disease Rate NewElysse PallagudÎncă nu există evaluări
- Balanced Diet: Bhavya Mds I Year Department of Conservative Dentistry & EndodonticsDocument76 paginiBalanced Diet: Bhavya Mds I Year Department of Conservative Dentistry & EndodonticsMayank AggarwalÎncă nu există evaluări
- Bone Tissue EngenieringDocument23 paginiBone Tissue EngenieringAna Emilia Holanda RolimÎncă nu există evaluări
- Temporomandibular DisordersDocument45 paginiTemporomandibular DisordersMohsin HabibÎncă nu există evaluări
- 5 PDFDocument8 pagini5 PDFoskar ORTIZÎncă nu există evaluări
- Rationale For Dental ImplantsDocument18 paginiRationale For Dental ImplantsSamir Nayyar100% (1)
- 2 Saliva PhysiologyDocument20 pagini2 Saliva PhysiologyvelangniÎncă nu există evaluări
- Pontics: Vaishakhi .Y. Baisane (Ivth Year B.D.S)Document47 paginiPontics: Vaishakhi .Y. Baisane (Ivth Year B.D.S)Vaishakhi BaisaneÎncă nu există evaluări
- Temporo Mandibular JointDocument60 paginiTemporo Mandibular JointchaitreeÎncă nu există evaluări
- Single Complete DentureDocument23 paginiSingle Complete DentureNelly SuriamahÎncă nu există evaluări
- Periodontal LigamentDocument47 paginiPeriodontal LigamentPrerna KrishanÎncă nu există evaluări
- Tooth Eruption TheoriesDocument9 paginiTooth Eruption Theoriesindian dental academyÎncă nu există evaluări
- Transitioning Patients From Teeth To ImplantsDocument11 paginiTransitioning Patients From Teeth To ImplantsAlexandra DumitracheÎncă nu există evaluări
- Implant Prosthodontics ParameterDocument4 paginiImplant Prosthodontics ParameterSorabh JainÎncă nu există evaluări
- Direct vs. Indirect Sinus Lift Procedure: A Comparison: March 2012Document8 paginiDirect vs. Indirect Sinus Lift Procedure: A Comparison: March 2012Sooraj SÎncă nu există evaluări
- Existing Restoration - Clinical Status: Secondary Caries Marginal Integrity Biomechanical FormDocument47 paginiExisting Restoration - Clinical Status: Secondary Caries Marginal Integrity Biomechanical FormDaniel WangÎncă nu există evaluări
- Introduction To ProsthodonticsDocument98 paginiIntroduction To ProsthodonticsmarwaÎncă nu există evaluări
- Dental Anatomy and PhysiologyDocument36 paginiDental Anatomy and PhysiologyCpt.WnchstrÎncă nu există evaluări
- Polyetheretherketone PEEK Dental Implants A Case FDocument8 paginiPolyetheretherketone PEEK Dental Implants A Case FPhoebe David100% (1)
- ANTI-PLAQUE-anticalculus AgentsDocument99 paginiANTI-PLAQUE-anticalculus Agentst sÎncă nu există evaluări
- Aging and PeriodontiumDocument9 paginiAging and PeriodontiumManushi Chauhan100% (2)
- The Use of Barium Sulfate For Implant TemplatesDocument4 paginiThe Use of Barium Sulfate For Implant TemplatesFreddy GarciaÎncă nu există evaluări
- CD Manual 2019Document107 paginiCD Manual 2019Jalil EnockÎncă nu există evaluări
- Anatomy of Gingiva and Um - Pros Tho Don Tic SignificanceDocument108 paginiAnatomy of Gingiva and Um - Pros Tho Don Tic SignificanceDilip Singh100% (1)
- Apexogenesis & ApexificationDocument35 paginiApexogenesis & ApexificationFaizan Ahmed50% (2)
- Holistic Approach To Full Mouth Rehab PDFDocument5 paginiHolistic Approach To Full Mouth Rehab PDFAna AlvaradoÎncă nu există evaluări
- Complete Rehabilitation of A Patient With Occlusal Wear PDFDocument7 paginiComplete Rehabilitation of A Patient With Occlusal Wear PDFsarfarazahmad19Încă nu există evaluări
- Postextraction Alveolar Ridge Preservation - Biological Basis and TreatmentsDocument12 paginiPostextraction Alveolar Ridge Preservation - Biological Basis and TreatmentsdorinkarakogluÎncă nu există evaluări
- Reducing The Risk of Failure Incomplete Denture PatientsDocument8 paginiReducing The Risk of Failure Incomplete Denture PatientsHisyam IshakÎncă nu există evaluări
- Tooth Wear, Etiology, Diagnosis and Its Management in Elderly: A Literature ReviewDocument0 paginiTooth Wear, Etiology, Diagnosis and Its Management in Elderly: A Literature ReviewmegamarwaÎncă nu există evaluări
- Teeth SettingDocument53 paginiTeeth Settingdoctor0002Încă nu există evaluări
- Thesis - Synopsis: Dr. Abhilash.ADocument12 paginiThesis - Synopsis: Dr. Abhilash.ARajesh SÎncă nu există evaluări
- 2015 Kin JIACD - Sticky Bone - Sohn Et Al PDFDocument20 pagini2015 Kin JIACD - Sticky Bone - Sohn Et Al PDFOscar CabreraÎncă nu există evaluări
- Removable Partial DentureDocument72 paginiRemovable Partial DentureAyodele Oludare AyodejiÎncă nu există evaluări
- Classification System For Oral Submucous FibrosisDocument6 paginiClassification System For Oral Submucous FibrosisMohamed FaizalÎncă nu există evaluări
- Preprosthetic Surgical ProceduresDocument57 paginiPreprosthetic Surgical ProceduresDentist Here100% (1)
- Rrrresidual Ridge ResorbtionDocument54 paginiRrrresidual Ridge Resorbtionsrinivaskalluri100% (1)
- Oral Diagnosis and Treatment Planning: Part 7. Treatment Planning For Missing TeethDocument11 paginiOral Diagnosis and Treatment Planning: Part 7. Treatment Planning For Missing TeethalfredoibcÎncă nu există evaluări
- DENTAL AUXILIARY EDUCATION EXAMINATION IN DENTAL MATERIALS: Passbooks Study GuideDe la EverandDENTAL AUXILIARY EDUCATION EXAMINATION IN DENTAL MATERIALS: Passbooks Study GuideÎncă nu există evaluări
- Bone Grafting Techniques for Maxillary ImplantsDe la EverandBone Grafting Techniques for Maxillary ImplantsÎncă nu există evaluări
- Geriatric Dentistry: Caring for Our Aging PopulationDe la EverandGeriatric Dentistry: Caring for Our Aging PopulationÎncă nu există evaluări
- Advancements in Casting Technology: Rapid Burnout InvestmentsDocument8 paginiAdvancements in Casting Technology: Rapid Burnout InvestmentsRajsandeep SinghÎncă nu există evaluări
- How To Remember ArticlesDocument7 paginiHow To Remember ArticlesRajsandeep SinghÎncă nu există evaluări
- 1 s2.0 S0022391315001377 MainDocument6 pagini1 s2.0 S0022391315001377 MainRajsandeep SinghÎncă nu există evaluări
- Interim Obturator Given in Aramany Class I DefectDocument14 paginiInterim Obturator Given in Aramany Class I DefectRajsandeep SinghÎncă nu există evaluări
- Overlay Denture 1Document9 paginiOverlay Denture 1api-3710948100% (1)
- Foreign Direct Investments (FDI)Document7 paginiForeign Direct Investments (FDI)Rajsandeep SinghÎncă nu există evaluări
- Pilates Stretches Hand OutDocument58 paginiPilates Stretches Hand OutRajsandeep SinghÎncă nu există evaluări
- Gupta Et Al-2014-Journal of ProsthodonticsDocument4 paginiGupta Et Al-2014-Journal of ProsthodonticsRajsandeep SinghÎncă nu există evaluări
- Facial NerveDocument5 paginiFacial NerveRajsandeep SinghÎncă nu există evaluări
- Pharyngeal ArchDocument6 paginiPharyngeal ArchRajsandeep SinghÎncă nu există evaluări
- Diagnosis and Treatment Planning For Edentulous or PotentiallyDocument73 paginiDiagnosis and Treatment Planning For Edentulous or PotentiallyRajsandeep SinghÎncă nu există evaluări
- Linear Coefficients of ExpansionDocument12 paginiLinear Coefficients of ExpansionVBT1Încă nu există evaluări
- The Physical Mechanisms of Complete Denture Retention: ProstheticsDocument5 paginiThe Physical Mechanisms of Complete Denture Retention: ProstheticsLisna K. RezkyÎncă nu există evaluări
- OcclusionDocument49 paginiOcclusionRajsandeep SinghÎncă nu există evaluări
- Growth and Dev TMJDocument76 paginiGrowth and Dev TMJRajsandeep Singh100% (2)
- Evaluation of Internal and Marginal Fit of Two Metal Ceramic System - in Vitro StudyDocument4 paginiEvaluation of Internal and Marginal Fit of Two Metal Ceramic System - in Vitro StudyRajsandeep SinghÎncă nu există evaluări
- Smart Phone For Shade Selection in Fixed ProsthodonticsDocument2 paginiSmart Phone For Shade Selection in Fixed ProsthodonticsRajsandeep SinghÎncă nu există evaluări
- Marginal Adaptation of Cast Partial Crowns Made of Pure Titanium and A Gold Alloy Under in Uence of A Manual Burnishing TechniqueDocument6 paginiMarginal Adaptation of Cast Partial Crowns Made of Pure Titanium and A Gold Alloy Under in Uence of A Manual Burnishing TechniqueRajsandeep SinghÎncă nu există evaluări
- 04 Retention, Stability and Support in Complete Denture Treatment - StudentsDocument51 pagini04 Retention, Stability and Support in Complete Denture Treatment - StudentsCookie CompÎncă nu există evaluări
- 4 - Ads - 14 - 033 Saliva in CdsDocument4 pagini4 - Ads - 14 - 033 Saliva in CdsRajsandeep SinghÎncă nu există evaluări
- 2013 Article 264 PDFDocument5 pagini2013 Article 264 PDFRajsandeep SinghÎncă nu există evaluări
- Ultraconservative Approach For Caries ManagementDocument12 paginiUltraconservative Approach For Caries ManagementRajsandeep SinghÎncă nu există evaluări
- Aaid Joi D 12 CL PDFDocument7 paginiAaid Joi D 12 CL PDFRajsandeep SinghÎncă nu există evaluări
- Development of FaceDocument77 paginiDevelopment of FaceRajsandeep SinghÎncă nu există evaluări
- Atrevievy of RootaresectivetherapyDocument19 paginiAtrevievy of RootaresectivetherapyRajsandeep SinghÎncă nu există evaluări
- Effect of Drugs On Oral Mucosa and Their ManagementDocument35 paginiEffect of Drugs On Oral Mucosa and Their ManagementRajsandeep Singh100% (1)
- Fur CationsDocument81 paginiFur CationsRajsandeep SinghÎncă nu există evaluări
- Final Project PDFDocument75 paginiFinal Project PDFuzzal ahmedÎncă nu există evaluări
- The Effect of Icariin On Bone Metabolism and Its Potential Clinical ApplicationDocument12 paginiThe Effect of Icariin On Bone Metabolism and Its Potential Clinical ApplicationBrenda MartinsÎncă nu există evaluări
- Ece 2010 AbstractsDocument316 paginiEce 2010 AbstractsClaudia IrimieÎncă nu există evaluări
- Osteoporosis PPT - LFP PDFDocument55 paginiOsteoporosis PPT - LFP PDFFarhan FauziÎncă nu există evaluări
- Atlas of Postmenopausal Osteoporosis 3rd Ed. - R. Rizzoli (CMG, 2010) WWDocument127 paginiAtlas of Postmenopausal Osteoporosis 3rd Ed. - R. Rizzoli (CMG, 2010) WWBrankoSalvariÎncă nu există evaluări
- Osteoporosis: A Review of Treatment Options: - February 2018 - Vol. 43 No. 2Document13 paginiOsteoporosis: A Review of Treatment Options: - February 2018 - Vol. 43 No. 2Sardono WidinugrohoÎncă nu există evaluări
- The Osteoimmunology of Alveolar Bone Loss: Connective Tissue Research March 2016Document24 paginiThe Osteoimmunology of Alveolar Bone Loss: Connective Tissue Research March 2016Khaled Al GhaebÎncă nu există evaluări
- Prolia PiDocument32 paginiProlia PiJoana JohnÎncă nu există evaluări
- Orthobullets Basic MODDocument172 paginiOrthobullets Basic MODNuno PaisÎncă nu există evaluări
- Filoteo, Angel Hannah A. BSN 3B: Pathophysiologic Process - RHEUMATOID ARTHRITISDocument1 paginăFiloteo, Angel Hannah A. BSN 3B: Pathophysiologic Process - RHEUMATOID ARTHRITISAngel FiloteoÎncă nu există evaluări
- Bone PathologyDocument78 paginiBone Pathologyanupama menonÎncă nu există evaluări
- TNF Superfamily and ILC2 Activation in Asthma by Takahiro Matsuyama, Brittany Marie Salter, Nahal Emami Fard, Kentaro Machida Androma SehmiDocument19 paginiTNF Superfamily and ILC2 Activation in Asthma by Takahiro Matsuyama, Brittany Marie Salter, Nahal Emami Fard, Kentaro Machida Androma SehmiTedÎncă nu există evaluări
- Ar 3595Document54 paginiAr 3595suryasanÎncă nu există evaluări
- Age-Dependent Biologic Response To Orthodontic Forces: Original ArticleDocument13 paginiAge-Dependent Biologic Response To Orthodontic Forces: Original ArticleAnushriya DuttaÎncă nu există evaluări
- Role of TFO in Progression of Periodontal DiseaseDocument11 paginiRole of TFO in Progression of Periodontal DiseaseNishtha KumarÎncă nu există evaluări
- Pathophysiology of OsteoporosisDocument6 paginiPathophysiology of OsteoporosisZenithaMeidaÎncă nu există evaluări
- Expression of Fibroblast Growth Factor 23, Vitamin D Receptor, and Sclerostin in Bone Tissue From Hypercalciuric Stone FormersDocument8 paginiExpression of Fibroblast Growth Factor 23, Vitamin D Receptor, and Sclerostin in Bone Tissue From Hypercalciuric Stone FormersVenansius Ratno KurniawanÎncă nu există evaluări
- Biology of OtmDocument19 paginiBiology of OtmNaveenÎncă nu există evaluări
- Chapter 80 Parathyroid Hormone, Calcitonin, Calcium and Phosphate Metabolism, Vitamin D, Bone, and TeethDocument12 paginiChapter 80 Parathyroid Hormone, Calcitonin, Calcium and Phosphate Metabolism, Vitamin D, Bone, and Teethputri aisheÎncă nu există evaluări
- Giant Cell Tumor of Bone - An Overview: Current Concepts ReviewDocument8 paginiGiant Cell Tumor of Bone - An Overview: Current Concepts ReviewDwi fitria nivaÎncă nu există evaluări
- HypercalcemiaDocument26 paginiHypercalcemiaPiya TangÎncă nu există evaluări
- Osteoporosis 2015 K RaceDocument37 paginiOsteoporosis 2015 K RaceRuzica PavlovicÎncă nu există evaluări
- Cells 10 02857 v2Document33 paginiCells 10 02857 v2DiegoÎncă nu există evaluări
- Principles of Periodontology Dentino - Et - Al-2013-Periodontology - 2000Document38 paginiPrinciples of Periodontology Dentino - Et - Al-2013-Periodontology - 2000Denisa FloreaÎncă nu există evaluări
- Frazier-Bowers Et Al, 2016Document11 paginiFrazier-Bowers Et Al, 2016Julio AbarzuaÎncă nu există evaluări
- Bone Remodeling: Cellular-Molecular Biology and Cytokine Rank-Rankl-Osteoprotegerin (Opg) System and Growth FactorsDocument9 paginiBone Remodeling: Cellular-Molecular Biology and Cytokine Rank-Rankl-Osteoprotegerin (Opg) System and Growth Factorssunshine bloomÎncă nu există evaluări
- These GNYUBKIN Vasily 2015Document151 paginiThese GNYUBKIN Vasily 2015AliÎncă nu există evaluări
- Osteoporosis: A.) Osteopenia B.) OsteoporosisDocument13 paginiOsteoporosis: A.) Osteopenia B.) OsteoporosisDale GoÎncă nu există evaluări