S-ar putea să vă placă și
- Gordons Functional PatternDocument9 paginiGordons Functional PatternKenneth Gabriel CatulinÎncă nu există evaluări
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicDe la EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicEvaluare: 5 din 5 stele5/5 (1)
- Drug StudyDocument2 paginiDrug StudyKristine YoungÎncă nu există evaluări
- Behavioral Health Care PlanDocument12 paginiBehavioral Health Care Planapi-520841770100% (1)
- History Taking: Item DescriptionDocument22 paginiHistory Taking: Item DescriptionBikash Sah100% (1)
- Illness ExpressionsDocument5 paginiIllness ExpressionsMichelle Susunaga RomeroÎncă nu există evaluări
- MSN SOAP Note TemplateDocument3 paginiMSN SOAP Note Templatexiomara torresÎncă nu există evaluări
- GIT Case ProformaDocument2 paginiGIT Case ProformaRiyaSinghÎncă nu există evaluări
- Rahaf Wardeh Internal Medicine 2016-2017Document4 paginiRahaf Wardeh Internal Medicine 2016-2017asdddÎncă nu există evaluări
- Physical Diagnosis: Nishalini RavindranDocument6 paginiPhysical Diagnosis: Nishalini RavindranShalini RavÎncă nu există evaluări
- NSG 300c Care Plan 1Document10 paginiNSG 300c Care Plan 1api-521018364Încă nu există evaluări
- CatapresDocument1 paginăCatapresCen Janber CabrillosÎncă nu există evaluări
- Case Presentation Station 3B Drug Study TramadolDocument3 paginiCase Presentation Station 3B Drug Study TramadolhahahahaaaaaaaÎncă nu există evaluări
- Chest Pain EvaluationDocument2 paginiChest Pain Evaluatione-MedTools100% (5)
- MaternalDocument29 paginiMaternalJim XieÎncă nu există evaluări
- Management of Patients With Special NeedsDocument4 paginiManagement of Patients With Special NeedsSophia MolinaÎncă nu există evaluări
- OSCESDocument4 paginiOSCESDemianaÎncă nu există evaluări
- Clinical Concept MapDocument5 paginiClinical Concept MapMj FernandezÎncă nu există evaluări
- A Comprehensive Neurological Examination Guide and Approach To LocalizationDocument86 paginiA Comprehensive Neurological Examination Guide and Approach To LocalizationLiberty AgcaoiliÎncă nu există evaluări
- This Study Resource Was: Assessment & Reasoning Cardiac SystemDocument6 paginiThis Study Resource Was: Assessment & Reasoning Cardiac SystemSharon TanveerÎncă nu există evaluări
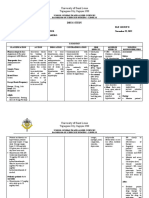
- I. Course Plan Unit TIM E (HR S) Objectives Content Teaching Learning Activities A.V. Aids Assessme NT MethodsDocument14 paginiI. Course Plan Unit TIM E (HR S) Objectives Content Teaching Learning Activities A.V. Aids Assessme NT MethodssimonjosanÎncă nu există evaluări
- Behavioral Health Care Plan: Assessment DataDocument9 paginiBehavioral Health Care Plan: Assessment Dataapi-521018364Încă nu există evaluări
- System Disorder: Active Learning TemplateDocument1 paginăSystem Disorder: Active Learning TemplateEli Reyes100% (1)
- NRN 202 Concept Map Patho-Altered Mental StatusDocument1 paginăNRN 202 Concept Map Patho-Altered Mental StatusWendy Gilbert50% (2)
- Eina History Physical 2010 VerticalDocument2 paginiEina History Physical 2010 Verticalgreenflames09Încă nu există evaluări
- Окклюзионная дизестзияDocument6 paginiОкклюзионная дизестзияАнна ЛужковскаяÎncă nu există evaluări
- Akash Presentation, NY2024Document13 paginiAkash Presentation, NY2024Akash ShahÎncă nu există evaluări
- Drug StudyDocument2 paginiDrug StudyKristine YoungÎncă nu există evaluări
- Bsn-Rs-Careplan 3-2Document12 paginiBsn-Rs-Careplan 3-2api-509646698Încă nu există evaluări
- Endo Confidential Health History PacketDocument6 paginiEndo Confidential Health History Packetalikhanomer5Încă nu există evaluări
- Drug Study Atenolol, Cefuroxime, SimvastatinDocument4 paginiDrug Study Atenolol, Cefuroxime, Simvastatinpaupaulala100% (4)
- The Neurologic HistoryDocument15 paginiThe Neurologic HistorythackeryuktaÎncă nu există evaluări
- Trans PMLS Pages 1 24Document17 paginiTrans PMLS Pages 1 24leexxjannelapatÎncă nu există evaluări
- Drug StudyDocument8 paginiDrug StudyChrizley Shawn DeroniaÎncă nu există evaluări
- OPD Adolescent History FormDocument5 paginiOPD Adolescent History FormNehemiah FranciscoÎncă nu există evaluări
- Audit FormsDocument4 paginiAudit Formsapi-349641525Încă nu există evaluări
- Drug Study: Anti-InfectiveDocument8 paginiDrug Study: Anti-InfectiveTri ShaÎncă nu există evaluări
- Adult Health Nursing IiDocument41 paginiAdult Health Nursing IiDiksha dudiÎncă nu există evaluări
- Connective TissueDocument4 paginiConnective TissuePaola Elizabeth González MartínezÎncă nu există evaluări
- Ściąga AnfDocument1 paginăŚciąga AnfKasia ManżukÎncă nu există evaluări
- College of Nursing: The Health Sciences CenterDocument3 paginiCollege of Nursing: The Health Sciences CenterAna Luisa Conejos ConeseÎncă nu există evaluări
- Clinical Skills in NeurologyDocument34 paginiClinical Skills in NeurologyHassen Kavi IsseÎncă nu există evaluări
- Drug Study Ob WardDocument7 paginiDrug Study Ob WardKc DichosoÎncă nu există evaluări
- Cerebral Palsy Note (SP Edit)Document1 paginăCerebral Palsy Note (SP Edit)medical chroniclesÎncă nu există evaluări
- SOAP Note NSG 6420 Week 8Document6 paginiSOAP Note NSG 6420 Week 8Jan FloydÎncă nu există evaluări
- Osce ReviewerDocument119 paginiOsce Reviewerchiaruuh tÎncă nu există evaluări
- Brand Name/ Generic Name Classification Action Indication Adverse Effect Contraindication Nursing Consideration Perennial Allergic RhinitisDocument4 paginiBrand Name/ Generic Name Classification Action Indication Adverse Effect Contraindication Nursing Consideration Perennial Allergic Rhinitisangel_witchie619Încă nu există evaluări
- finalsURINARY ELIMINATION DIAGNOSTICSDocument11 paginifinalsURINARY ELIMINATION DIAGNOSTICSFrances LiqueÎncă nu există evaluări
- Synapse in My Pocket Neuro Exam & Localization - 1st Ed 2020Document63 paginiSynapse in My Pocket Neuro Exam & Localization - 1st Ed 2020SnowyÎncă nu există evaluări
- SOAP - Blank - Template Word Doc 2022Document6 paginiSOAP - Blank - Template Word Doc 2022Joan McutestÎncă nu există evaluări
- E/M Audit Form: Chart #Document2 paginiE/M Audit Form: Chart #Sakshi BishnoiÎncă nu există evaluări
- Concept Map 10 25 23 RachelDocument1 paginăConcept Map 10 25 23 Rachelapi-726698459Încă nu există evaluări
- Back Pain in Children and AdolescentsDocument11 paginiBack Pain in Children and AdolescentsBariša KiršnerÎncă nu există evaluări
- Resident Guide To Pediatric Rheumatology 2011Document61 paginiResident Guide To Pediatric Rheumatology 2011Ana HinicÎncă nu există evaluări
- ADULT HEALTH NURSING-2 INCLUDING GERIATRIC NURSING (Syllabus)Document4 paginiADULT HEALTH NURSING-2 INCLUDING GERIATRIC NURSING (Syllabus)Abhishek NaharÎncă nu există evaluări
- Palmitoylethanolamide (PEA)Document4 paginiPalmitoylethanolamide (PEA)Qwerty QwertyÎncă nu există evaluări
- CNS: Headache, InsomniaDocument5 paginiCNS: Headache, InsomniaDave FagaritaÎncă nu există evaluări
- Neftali de La Cruz EmeterioDocument2 paginiNeftali de La Cruz EmeterioNeftali EmeterioÎncă nu există evaluări
- Neftali de La Cruz EmeterioDocument2 paginiNeftali de La Cruz EmeterioNeftali EmeterioÎncă nu există evaluări
- Who Health System Building BlocksDocument2 paginiWho Health System Building BlocksPiny Elleine CesarÎncă nu există evaluări
- Medical Jurisprudence Chapters 1-4 PDFDocument42 paginiMedical Jurisprudence Chapters 1-4 PDFPiny Elleine CesarÎncă nu există evaluări
- Legal Medicine by Pedro SolisDocument792 paginiLegal Medicine by Pedro SolisNLainie Omar100% (3)
- Legal Medicine by Pedro SolisDocument792 paginiLegal Medicine by Pedro SolisNLainie Omar100% (3)
- Medicines, 6th EdDocument609 paginiMedicines, 6th EdNguyễn Sanh Luật50% (2)
- Research Article Respiratory RelatedDocument3 paginiResearch Article Respiratory RelatedRizza Faye BalayangÎncă nu există evaluări
- First Aid QuizDocument5 paginiFirst Aid QuizIan AriÎncă nu există evaluări
- CancerDocument70 paginiCancerapi-3735995100% (1)
- Eye & ENTDocument12 paginiEye & ENTShandar SadafÎncă nu există evaluări
- A Presentation On Congenital HyperthyroidismDocument26 paginiA Presentation On Congenital Hyperthyroidismkriti kaushalÎncă nu există evaluări
- Jtptunimus GDL Handayanig 5251 2 Bab2Document42 paginiJtptunimus GDL Handayanig 5251 2 Bab2Rendra Syani Ulya FitriÎncă nu există evaluări
- National Training Program On GDDDocument4 paginiNational Training Program On GDDshakkiryousufÎncă nu există evaluări
- Monthly Wellness Tip Heat StressDocument1 paginăMonthly Wellness Tip Heat StressbharathaninÎncă nu există evaluări
- Complication of Blood TransfusionDocument5 paginiComplication of Blood TransfusionChey Ochy ApriliaÎncă nu există evaluări
- Bilateral Peritonsillar AbscessDocument5 paginiBilateral Peritonsillar AbscessRadu BonaciuÎncă nu există evaluări
- Jurnal Forensik Trauma KimiaDocument5 paginiJurnal Forensik Trauma Kimiaikram hanafiÎncă nu există evaluări
- Jurnal 3Document4 paginiJurnal 3Arum RaniÎncă nu există evaluări
- A Technical Seminar Presentation On: Bionic EyeDocument13 paginiA Technical Seminar Presentation On: Bionic EyeRohith AddagatlaÎncă nu există evaluări
- Contoh Form IDODocument62 paginiContoh Form IDOOki Vera UntariÎncă nu există evaluări
- Curriculum Vitae: Personal DetailsDocument3 paginiCurriculum Vitae: Personal DetailskadekÎncă nu există evaluări
- Dnrle Influenza NCPDocument3 paginiDnrle Influenza NCPEna RodasÎncă nu există evaluări
- Urostomy Guide - American Cancer SocietyDocument19 paginiUrostomy Guide - American Cancer SocietyDipa HandraÎncă nu există evaluări
- Approach To Floppy InfantDocument44 paginiApproach To Floppy InfantNavya Hegde100% (2)
- Test Bank For Nursing Assistant A Nursing Process Approach 11th EditionDocument7 paginiTest Bank For Nursing Assistant A Nursing Process Approach 11th EditionLarry Cessor100% (26)
- Assesment Preop - Rohemi 28.09.21Document27 paginiAssesment Preop - Rohemi 28.09.21Reza Devianto HambaliÎncă nu există evaluări
- PB-00823 - Rev001 - SuperSonic MACH 40 BrochureDocument8 paginiPB-00823 - Rev001 - SuperSonic MACH 40 Brochuresoyuzmedimaging and diagnostics ltdÎncă nu există evaluări
- Effects of Vernonia Amygdalina (Bitter Leaf) On The Bio-Marker of Oxidative Stress in Accetaminophen Induced Liver Damage of Albino RatsDocument12 paginiEffects of Vernonia Amygdalina (Bitter Leaf) On The Bio-Marker of Oxidative Stress in Accetaminophen Induced Liver Damage of Albino Ratsiaset123Încă nu există evaluări
- Farmakologi Cns Stimulants DrugsDocument15 paginiFarmakologi Cns Stimulants DrugsRifqiÎncă nu există evaluări
- Covid19 - Pathophysiology and ManagementDocument51 paginiCovid19 - Pathophysiology and ManagementMyraflor CaroÎncă nu există evaluări
- Description:: Dance Therapy "In The Mood of Dancing"Document2 paginiDescription:: Dance Therapy "In The Mood of Dancing"kristine_silangÎncă nu există evaluări
- Precautions - Isolation Precautions - Guidelines Library - Infection Control - CDCDocument6 paginiPrecautions - Isolation Precautions - Guidelines Library - Infection Control - CDCKomite PPI RSUDPCÎncă nu există evaluări
- Apollo Fertility IUI IVF Clinic and Dr. Lakshmi Krishna Leela GynecologistDocument6 paginiApollo Fertility IUI IVF Clinic and Dr. Lakshmi Krishna Leela GynecologistPrabha SharmaÎncă nu există evaluări
- Caroline Stone. Osteopathic ApproachDocument54 paginiCaroline Stone. Osteopathic ApproachIoan Andra100% (5)
- nsg-320cc Care Plan 1Document14 pagininsg-320cc Care Plan 1api-509452165Încă nu există evaluări
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDe la EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsÎncă nu există evaluări
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDe la EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisEvaluare: 4.5 din 5 stele4.5/5 (42)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeEvaluare: 2 din 5 stele2/5 (1)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDe la EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsEvaluare: 5 din 5 stele5/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe la EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityEvaluare: 4 din 5 stele4/5 (24)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDe la EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedEvaluare: 5 din 5 stele5/5 (80)
- The Obesity Code: Unlocking the Secrets of Weight LossDe la EverandThe Obesity Code: Unlocking the Secrets of Weight LossEvaluare: 4 din 5 stele4/5 (6)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDe la EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDe la EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsEvaluare: 4.5 din 5 stele4.5/5 (169)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDe la EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDEvaluare: 5 din 5 stele5/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDe la EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityEvaluare: 4 din 5 stele4/5 (3)
- Gut: the new and revised Sunday Times bestsellerDe la EverandGut: the new and revised Sunday Times bestsellerEvaluare: 4 din 5 stele4/5 (392)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDe la EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeEvaluare: 4.5 din 5 stele4.5/5 (253)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDe la EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsEvaluare: 3.5 din 5 stele3.5/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisDe la EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisEvaluare: 3.5 din 5 stele3.5/5 (2)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningDe la EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningEvaluare: 4 din 5 stele4/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.De la EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Evaluare: 4.5 din 5 stele4.5/5 (110)
- To Explain the World: The Discovery of Modern ScienceDe la EverandTo Explain the World: The Discovery of Modern ScienceEvaluare: 3.5 din 5 stele3.5/5 (51)
- An Autobiography of Trauma: A Healing JourneyDe la EverandAn Autobiography of Trauma: A Healing JourneyEvaluare: 5 din 5 stele5/5 (2)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDe la EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessEvaluare: 4.5 din 5 stele4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDe la EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisEvaluare: 4 din 5 stele4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDe la EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryEvaluare: 4 din 5 stele4/5 (44)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisDe la EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisEvaluare: 4 din 5 stele4/5 (9)