S-ar putea să vă placă și
- General Anesthesia For C-SectionDocument4 paginiGeneral Anesthesia For C-SectionardiÎncă nu există evaluări
- An Algorithmic Approach To Low Back PainDocument8 paginiAn Algorithmic Approach To Low Back PainardiÎncă nu există evaluări
- Clinical Presentation of LastDocument7 paginiClinical Presentation of LastardiÎncă nu există evaluări
- Checklist For Local Anesthetic Toxicity Treatment 1-18-12Document2 paginiChecklist For Local Anesthetic Toxicity Treatment 1-18-12Akilesh RamasamyÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (72)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- 11 - Effective Pages: Beechcraft CorporationDocument80 pagini11 - Effective Pages: Beechcraft CorporationCarlos Andres Oviedo OsorioÎncă nu există evaluări
- Scheda Tecnica-Golf GTEDocument1 paginăScheda Tecnica-Golf GTEBlogo MotoriÎncă nu există evaluări
- English ESP Mapeh Filipino Aral. Pan. Math Mtb/Mle English ESP Mapeh Filipino Aral. Pan. Math Mtb/MleDocument2 paginiEnglish ESP Mapeh Filipino Aral. Pan. Math Mtb/Mle English ESP Mapeh Filipino Aral. Pan. Math Mtb/MleJackielou Biala-Guba Mosada RebualosÎncă nu există evaluări
- Adidas Suns CatalogDocument59 paginiAdidas Suns Catalogstumap8441Încă nu există evaluări
- Running With CeruttyDocument32 paginiRunning With Ceruttyviveksharma666100% (1)
- EVOBET88 Situs Judi Slot Online Gacor Dan Agen Judi Bola PDFDocument1 paginăEVOBET88 Situs Judi Slot Online Gacor Dan Agen Judi Bola PDFArrafi FahrezaÎncă nu există evaluări
- DC-3 - Recovery Software Guide - V06 04 00 5465 - ECD117-1Document20 paginiDC-3 - Recovery Software Guide - V06 04 00 5465 - ECD117-1ДмитрийÎncă nu există evaluări
- IELTS-Reading-Writing-7-8-Not Edititing VersionDocument134 paginiIELTS-Reading-Writing-7-8-Not Edititing VersionMd. Anwar HossainÎncă nu există evaluări
- Planeta ComicDocument31 paginiPlaneta ComicDavid ZxsÎncă nu există evaluări
- Today MagDocument35 paginiToday MagSofía BerrotaránÎncă nu există evaluări
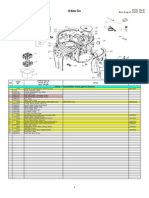
- Saeco Odea GoDocument8 paginiSaeco Odea GotomitadanielÎncă nu există evaluări
- PriceList 201120Document1 paginăPriceList 201120KorRhinoÎncă nu există evaluări
- WWI 32nd Infantry DivisionDocument77 paginiWWI 32nd Infantry DivisionCAP History LibraryÎncă nu există evaluări
- Manteniment R290 R190 PDFDocument13 paginiManteniment R290 R190 PDFJoan Pladeveya SelvasÎncă nu există evaluări
- Oaklawn Park: Daily Racing FormDocument40 paginiOaklawn Park: Daily Racing FormReille VanderÎncă nu există evaluări
- La Espada Del Tiempo Rick RiordanDocument320 paginiLa Espada Del Tiempo Rick RiordanRafael VargasÎncă nu există evaluări
- Catalogo COMFORSIL SiliconasDocument51 paginiCatalogo COMFORSIL SiliconasTalquipen DbzapÎncă nu există evaluări
- Electrical Resistant Heavy Duty Safety Shoes With MidsoleDocument3 paginiElectrical Resistant Heavy Duty Safety Shoes With MidsoleEunice GayetaÎncă nu există evaluări
- Runner - World - UK - 2014 (GTRG) PDFDocument116 paginiRunner - World - UK - 2014 (GTRG) PDFhocusÎncă nu există evaluări
- FC Steaua BucureștiDocument27 paginiFC Steaua BucureștiRikky2403xÎncă nu există evaluări
- Exercies For Lower BackDocument2 paginiExercies For Lower BackAnkush RatanpalÎncă nu există evaluări
- 100 ESL Board Games PreviewDocument10 pagini100 ESL Board Games PreviewAmrah AmrahovÎncă nu există evaluări
- F 1 C 1Document2 paginiF 1 C 1Abel Gonzalez100% (7)
- AerobicsDocument8 paginiAerobicsIvan Dennis SalupanÎncă nu există evaluări
- Construction and Working:: Porter GovernorDocument5 paginiConstruction and Working:: Porter Governoraverify53Încă nu există evaluări
- Falls From LaddersDocument3 paginiFalls From Laddersao185029Încă nu există evaluări
- Wonderwall Chord Progression Song LyricsDocument2 paginiWonderwall Chord Progression Song LyricsJames WatsonÎncă nu există evaluări
- 2022 Hawaii Hall of HonorDocument1 pagină2022 Hawaii Hall of HonorHonolulu Star-AdvertiserÎncă nu există evaluări
- Short Story CinderellaDocument2 paginiShort Story CinderellaInbar Surya Seru0% (1)
- Season3 PKL DATA FOR DATA ANALYTICSDocument3 paginiSeason3 PKL DATA FOR DATA ANALYTICSBhagya SreeÎncă nu există evaluări