Gineco.
eu [13] 145-147 [2017]
gineco
DOI: 10.18643/gieu.2017.145
@ 2017 Romanian Society of Ultrasonography in Obstetrics and Gynecology
case reports eu
Advanced colorectal cancer
in young, HIV positive woman.
Case report
Abstract Sergiu Chirilă1,
Leonard Gurgaș1,
Colorectal cancer is one of the most common forms of cancers, having a higher incidence ratio in the case of human
immunodeficiency virus (HIV) infected population in comparison with the general population. Identifying cases where Ionuț G. Revnic2,
cancer develops in HIV positive patients is important, as studies demonstrate that, under treatment, HIV positive patients Mihaela
have the same prognostic as HIV negative patients. We present the case of a 24-year-old HIV infecteced woman diagnosed Zamfirescu1,
with rectal adenocarcinoma with liver metastasis, with history of oral contraceptive pills. The neoplasia was in an inoperable Tony L. Hangan1
stage, therefore, the therapeutical action was chemotherapy. The contraceptive therapy was stopped immediately after
diagnosis, while specific therapy for HIV infection was added later in the evolution of the disease, due to late discovery. 1. Faculty of Medicine,
University “Ovidius”
The health status of the patient had a rapid degradation. Due to the increasing incidence of all types of cancers in the HIV of Constanța, Romania
positive population, especially affecting young people, and based on oral contraceptive intake, it is worth studying further 2. Polaris Medical Hospital,
Sugeacu, Cluj-Napoca,
if screening for HIV infection in patients diagnosed with different forms of cancers has an effect on their survival rate. Romania
Keywords: HIV, rectal neoplasms, neoplasm metastasis, diagnosis
Correspondence:
Drd. Leonard Gurgas
e-mail: leonard.gurgas11@
gmail.com
Introduction alpha-fetoprotein test (0.82 ng/mL). CA 125 and CA 15-3
Among gastrointestinal neoplastic diseases, colorectal were within normal values.
cancer is proven to have the highest incidence in Constanta At the initial control, general status was good, with pale
County(1) among gastrointestinal cancers, representing teguments and mucosa, blood pressure 110/60 mmHg,
more than 60% of the cases. For patients below 18 years, heart rate 80bpm. The abdomen was mobile with the bre-
these represent 17% of the cases recorded in recent years(1). athing, sensible at palpation in the right hypochondrium.
Other studies, conducted in the same geographical area, The liver could be identified 2 cm below the costal rebord.
or at international level, indicate a significantly higher Upper gastrointestinal endoscopy was performed with no
incidence of all types of neoplastic diseases in the case pathological modifications of the esophagus, stomach
of patients infected with human immunodeficiency virus and first two parts of the duodenum.The patients was
(HIV)(2,3), and for colorectal cancer(4). also in treatment starting from 3 years ago with oral
We present a case of advanced, metastatic colorectal contraceptives.
cancer in a 24-year-old woman on oral contraceptives. Abdominal contrast computed tomography (CT) has
The awareness of the increased risk of cancers for patients been conducted. This revealed liver with a longitudinal
infected with HIV is very important, as it represents an diameter of the right hepatic lobe of 240 mm, with in-
emerging health problem. homogeneous structure caused by macronodular structu-
res with irregular contour, with hypodense signal and dis-
Case Report crete calcifications. Multiple lesions were identified when
We present the case of a 24-year-old woman, diagnosed contrast substances were used, localized at the level of
with colorectal cancer. The debut of the symptomato- both hepatic lobes. The largest mass was 108mm/106mm,
logy was with discomfort and pain in the right hypo- localized in the IVa, VII and VIII segments, which invades
chondrium area. This was the reason for the patient to the right hepatic canal, with dilatation before the intra-
present for consultation at her Family Medicine Office hepatic biliary canal. Thrombosis of the posterior ram
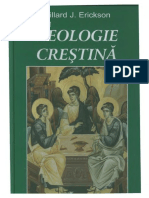
from Constanta. The first investigation conducted was of the portal vein was also observed (Figures 1 and 2).
an ultrasonographic scan. The investigation revealed two Other findings include a normal gallbladder, increased
inhomogenous masses of 4-5 cm each, with increased splenic size 105mm/55mm/185mm, portal vein with a cali-
splenic size 15.5cm/4.8cm, and an undetermined mass ber of 13mm, pancreas, suprarenal glands and kidneys with
located in the pelvic area 4.5cm/5cm. anormal aspect. The uterus, ovaries and the bladder present
Received:
Blood tests showed severe anemia, with hemoglobin no signs of abnormalities. Multiple adenopathies with maxi- October 22, 2017
values of 7 g/dl and very high values for carcinoembryo- mal diameters between 15mm and 21mm were identified. Revised:
November 05, 2017
nic antigen (1538.6 ng/ml), cancer antigen (CA) 19-9 Because the findings from the CT didn’t match the re- Accepted:
(72458.17 U/ml) and higher than normal values for the sults of the blood tests conducted before, a colonoscopy November 26, 2017
Vol. 13 • No. 50 (4/2017)
145
Chirilă et al. Advanced colorectal cancer in young, HIV positive woman
Figure 1. Macronodular mass Figure 2. Multiple disseminated masses
was performed. This identified a proliferative, excentric A second colonoscopy was conducted. A rigid, ulcerative,
bleeding mass, localized at the level of the rectal canal. hemorrhagic mass is observed in one side of the lumen
Four fragments were taken for anatomopathological of the rectum, within 3-4 cm of the anal canal (Figure 4).
examination. The conclusions of the investigations were that the
The immediate treatment consisted of three erythrocyte tumor is inoperable, therefore, chemotherapy with FOL-
mass transfusions, increasing the hemoglobin at 8.8 g/dl, FOX (Leucovorin Calcium, Fluorouracil, Oxaliplatin). The
iron sucrose injections with a favorable clinical evolution. first course was well tolerated with the improvement
Discharge diagnoses were: rectal malignant neoplasm of of the symptomatology. Starting with the third course,
rectum, secondary malignant neoplasm of liver, anemia. bevacizumab was added.
At home, and during the third day of hospitalization the After the results for the mutation KRAS, NRAS, BRAF
patient presents episodes of fever. came back negative, the recommendation for cetuximab,
The result from the histopathological tests identify starting with the sixth cure was made.
characteristics of intestinal adenocarcinoma associated After another three cures of chemotherapy, the patient
with intraepithelial neoplastic lesions. The grade of the decides to undergo further investigations and treatment in
tumor remains undetermined. another clinic. A new CT scan was conducted. This reveals
After approximately three weeks, the patients asked an increased hepatic size, with inhomogeneous structure,
for a second opinion from an oncology specialized clinic. important splenomegaly, and numerousadenopathies.
The patient undergone (positron emission tomography) The patient presents fever episodes, with no specific
PET-CT scan with the purpose of staging, magnetic reso- symptomatology, with negative hem cultures, urinalysis,
nance imaging (MRI) of the abdomen, colonoscopy and MRSA and ESBL screening being negative. Because the
gene mutation testing were performed for BRAF V600, discrepancy between the clinical and imagistic hepatic
KRAS, and NRAS. aspect and the neoplastic disease, a liver biopsy was done
The PET-CT scan revealed abnormally increased uptake and also tests for infectious diseases (HIV, hepatitis B
of F-18 fluorodeoxyglucose (FDC) in the lymph node, virus and hepatitis C virus). The result of the HIV testing
within the right pericardiac area, with a diameter of 20.1 was positive (i.e. rapid test and ELISA confirmation test).
mm. Abnormal increase of FDC uptake was also pre- Following the recommendations, the patient was ad-
sent in the bowel segment, in the rectum, with a circular mitted to the Infectious Diseases clinic where HIV infecti-
thickening, compatible with malignant tissue. Multiple on is confirmed, with stage C3 acquired immunodeficiency
lesions in both lobes of the liver parenchyma with sizes syndrome. Antiretroviral therapy was indicated.
significantly larger compared to the previous data from The patient died within the next two weeks due to
the CT (Figure 3). multiple organ insufficiencies, with hepatic insufficiency.
The whole abdomen MRI concluded that the tumoral
mass is 4 cm far from the anal verge, localizes anteri- Discussion
orly in the rectum, with the craniocaudal size of 29 mm, The particularities of the case are the rapid evolution
transverse 33 mm, AP 10 mm, without extension towards of the disease, the young age of the patient and the
perirectal fatty tissues, with perirectal lymph node up to association of oral contraceptives which at admission
7 mm in diameter. it were stop and HIV infection. The early age of the
146 Vol. 13 • No. 50 (4/2017)
Chirilă et al. Advanced colorectal cancer in young, HIV positive woman gineco
eu
patient and the aggressive course of the disease was
reported before, but this happened before the era of
highly active antiretroviral therapies (HAART)(5). In
the case presented, the patient was untreated for HIV,
therefore, the similarities with cases presented before
HAART it was very likely to appear.
Significant published studies(6,7) demonstrate the fact
that anal and colorectal cancer has a significantly higher
incidence in people infected with HIV, and especially in
the case of men who have sex with men. At the same
time, if HIV positive patients with neoplastic diseases
receive proper ARV treatment, their survival rate is
similar to the one observed in the general population(8).
Also, the possibility of using both types of substances,
for the treatment of HIV - with HAART and neoplasia
with different chemotherapies was assessed, and the
results show that both treatments retain their efficacy
and safety(9,10).
The purpose of this case presentation is to increase
the awareness that non-communicable diseases become
a real burden on the HIV positive population, as people Figure 3. PET-CT Scan with increased uptake liver and rectal areas
living with HIV infection have a higher life expectancy
nowadays due to advances on the treatment. Also,
because neoplastic diseases have a higher incidence in
the HIV positive population(11), screening for HIV on
patients diagnosed with different neoplastic diseases,
especially the ones frequently found, like pulmonary
cancers(12,13), colorectal cancers(4,14), anal cancer(15). A
study conducted in Korea showed a twofold prevalen-
ce of HIV infection in the case of patients diagnosed
with colorectal cancer(16), results confirmed by other
studies(17).
Conclusions
Due to the increasing incidence of cancers in the HIV
positive population, especially affecting young people, and
based on oral contraceptive intake it is worth studying
further if screening for HIV infection in patients diagno-
sed with different forms of cancers has an effect on their
survival rate. n Figure 4. Tumoral mass in the rectum
1. Severin B, Adumitresei C, Damaschin F, Broască V, Chirilă S, Mocanu E. Particularităţi 10. Berretta M, Lleshi A, Zanet E, Bearz A, Simonelli C, Fisichella R, et al. Bevacizumab
References
Privind Evoluţia Neoplaziilor în Judeţul Constanţa, în Perioada 2010-2013. Public plus irinotecan-, fluorouracil-, and leucovorin-based chemotherapy with concomitant
Health, Economy and Management in Medicine 2015, 3(60), 25-7. HAART in an HIV-positive patient with metastatic colorectal cancer. Onkologie 2008,
2. Chirila S, Hangan LT, Rugina S. Cancer incidence in HIV patients under HAART 31(7), 394-7.
therapy in a HIV-1 F1 subtype endemic area. ARS Medica Tomitana 2015, 217. 11. Park LS, Hernandez-Ramirez RU, Silverberg MJ, Crothers K, Dubrow R. Prevalence
3. Hessol NA, Strickler HD. Cancer risk in people living with HIV. Lancet HIV 2017, 4(11), of non-HIV cancer risk factors in persons living with HIV/AIDS: a meta-analysis. AIDS
e477-e9. 2016, 30(2), 273-91.
4. O’Neill TJ, Nguemo JD, Tynan A-M, Burchell AN, Antoniou T. Risk of Colorectal Cancer 12. Cambrea Simona C, Resul G, Danteș E, Halichidis S, Chirilă S. Invasive Lung
and Associated Mortality in HIV: A Systematic Review and Meta-Analysis. JAIDS Adenocarcinoma Mimicking Nodular Tuberculosis in a HIV Positive Patient (Case
Journal of Acquired Immune Deficiency Syndromes. 2017, 75(4), 439-47. report). ARS Medica Tomitana 2015, 75.
5. Klugman AD, Schaffner J. Colon adenocarcinoma in HIV infection: a case report and 13. Mena A, Meijide H, Marcos PJ. Lung Cancer in HIV-Infected Patients. AIDS Rev 2016,
review. Am J Gastroenterol. 1994, 89(2), 254-6.
18(3), 138-44.
6. Machalek DA, Poynten M, Jin F, Fairley CK, Farnsworth A, Garland SM, et al. Anal
14. Silverberg MJ, Chao C, Leyden WA, Xu L, Horberg MA, Klein D, et al. HIV infection,
human papillomavirus infection and associated neoplastic lesions in men who have
immunodeficiency, viral replication, and the risk of cancer. Cancer Epidemiol
sex with men: a systematic review and meta-analysis. Lancet Oncol. 2012, 13(5),
487-500. Biomarkers Prev 2011, 20(12), 2551-9.
7. Keller SC, Momplaisir F, Lo Re V, Newcomb C, Liu Q, Ratcliffe SJ, et al. Colorectal 15. Bower M, Powles T, Newsom-Davis T, Thirlwell C, Stebbing J, Mandalia S, et al.
cancer incidence and screening in US Medicaid patients with and without HIV HIV-Associated Anal Cancer: Has Highly Active Antiretroviral Therapy Reduced the
infection. AIDS Care 2014, 26(6), 716-22. Incidence or Improved the Outcome? JAIDS Journal of Acquired Immune Deficiency
8. Alfa-Wali M, Allen-Mersh T, Antoniou A, Tait D, Newsom-Davis T, Gazzard B, et al. Syndromes. 2004, 37(5), 1563-5.
Chemoradiotherapy for anal cancer in HIV patients causes prolonged CD4 cell count 16. Kee MK, Hwang DY, Lee JK, Kim SH, Chu C, Lee JH, et al. Estimation of HIV
suppression. Ann Oncol 2012, 23(1):, -7. Seroprevalence in Colorectal Hospitals by Questionnaire Survey in Korea, 2002-2007.
9. Berretta M, Lleshi A, Cappellani A, Bearz A, Spina M, Talamini R.et al. Oxaliplatin Osong Public Health Res Perspect. 2011, 2(2):, -8.
based chemotherapy and concomitant highly active antiretroviral therapy in the 17. Traore B, Bah TS, Traore FA, Sow MS, Diane S, Keita M, et al. The Prevalence of HIV
treatment of 24 patients with colorectal cancer and HIV infection. Curr HIV Res 2010, in Cancer Patients at the Surgical Oncology Unit of Donka University Hospital of
8(3), 218-22. Conakry (Guinea). Journal of Cancer Epidemiology 2015, 2015, 4.
Vol. 13 • No. 50 (4/2017)
147
S-ar putea să vă placă și
- Encyclopedia of Neurological Sciences (5 Vols) - M. Aminoff, R. Daroff (Elsevier, 2003) WWDocument4.334 paginiEncyclopedia of Neurological Sciences (5 Vols) - M. Aminoff, R. Daroff (Elsevier, 2003) WWlgÎncă nu există evaluări
- Mcs M 1Document31 paginiMcs M 1Corina DrutaÎncă nu există evaluări
- Seminar 6Document10 paginiSeminar 6lgÎncă nu există evaluări
- Reading Comprehension: Tiger Mother Was A Funny, Apologetic, Self-Knowing Memoir Recounting Chua's HyperdemandingDocument9 paginiReading Comprehension: Tiger Mother Was A Funny, Apologetic, Self-Knowing Memoir Recounting Chua's HyperdemandinglgÎncă nu există evaluări
- Seminar 6Document10 paginiSeminar 6lgÎncă nu există evaluări
- Cinemat PMDocument1.053 paginiCinemat PMlgÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- HTTP Healthmedicinet Com II 2013 11 PDFDocument324 paginiHTTP Healthmedicinet Com II 2013 11 PDFtuni santeÎncă nu există evaluări
- Summary SecondANDl SetDocument57 paginiSummary SecondANDl SetPetros TemboÎncă nu există evaluări
- 4 HivDocument33 pagini4 HivAmr KhayyalÎncă nu există evaluări
- Sociodemographic Characteristics of Patients With Advanced HIV Disease in Enugu, South-East Nigeria: A Retrospective Analysis of Program DataDocument6 paginiSociodemographic Characteristics of Patients With Advanced HIV Disease in Enugu, South-East Nigeria: A Retrospective Analysis of Program DataInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Antimicrobial StewardshipDocument19 paginiAntimicrobial StewardshipFelipe VicenteñoÎncă nu există evaluări
- South African Early Childhood Review 2019Document52 paginiSouth African Early Childhood Review 2019Mail and GuardianÎncă nu există evaluări
- Medical-Surgical Nursing Assessment and Management of Clinical Problems 9e Chapter 7Document5 paginiMedical-Surgical Nursing Assessment and Management of Clinical Problems 9e Chapter 7sarasjunkÎncă nu există evaluări
- Characteristics of Gay, Bisexual and Other Men Who.1 PDFDocument6 paginiCharacteristics of Gay, Bisexual and Other Men Who.1 PDFGvidas MikalauskasÎncă nu există evaluări
- Avexa Annual Report 2013Document64 paginiAvexa Annual Report 2013shoaiba1Încă nu există evaluări
- Kualitas Hidup ODHADocument13 paginiKualitas Hidup ODHAAchmad VindoÎncă nu există evaluări
- STEP 1 Could It Be HIV? STEP 2 Informed Consent and Testing STEP 3 Conveying Test ResultsDocument2 paginiSTEP 1 Could It Be HIV? STEP 2 Informed Consent and Testing STEP 3 Conveying Test ResultsahjkseflhasefÎncă nu există evaluări
- 627 1196 1 PBDocument7 pagini627 1196 1 PBannisa dian zizianiÎncă nu există evaluări
- Mompati Letsweletse Hiv Case 20110183Document25 paginiMompati Letsweletse Hiv Case 20110183Mompati LetsweletseÎncă nu există evaluări
- Antiviral Agents and Infection ControlDocument94 paginiAntiviral Agents and Infection ControlKimberly GeorgeÎncă nu există evaluări
- Zimbabwe OSDM Webrevised 2017Document116 paginiZimbabwe OSDM Webrevised 2017Richard Makurumidze Senior0% (1)
- Characteristics, Prevention, and Management of Cardiovascular Disease in People Living With HIV - AHA 2019Document27 paginiCharacteristics, Prevention, and Management of Cardiovascular Disease in People Living With HIV - AHA 2019Michael Amarillo CorreaÎncă nu există evaluări
- Clinical Management of TB and HIVDocument154 paginiClinical Management of TB and HIVapi-3781623100% (3)
- Antiviral Agents: Unit - 2 Pharmaceutical Chemistry - I (Advanced Medicinal Chemistry) Topic: Antiviral AgentsDocument20 paginiAntiviral Agents: Unit - 2 Pharmaceutical Chemistry - I (Advanced Medicinal Chemistry) Topic: Antiviral AgentsGunjan Kalyani100% (1)
- ADS 312 Additional Help Document: GH/OHA/SCMS "Restricted Commodity" Approval of PharmaceuticalsDocument7 paginiADS 312 Additional Help Document: GH/OHA/SCMS "Restricted Commodity" Approval of PharmaceuticalsBrunoRibeiroÎncă nu există evaluări
- Final Proposal Based On CommentsDocument51 paginiFinal Proposal Based On CommentsWudu Sewmehon100% (1)
- HIV and AIDSDocument75 paginiHIV and AIDSMarc Imhotep Cray, M.D.100% (1)
- Hetero Corp Presentation 2016Document23 paginiHetero Corp Presentation 2016Evan TanswariÎncă nu există evaluări
- Journalists Guide 2013Document204 paginiJournalists Guide 2013RomeMUN2013Încă nu există evaluări
- Essentials of Diagnostics WhitepaperDocument9 paginiEssentials of Diagnostics WhitepaperDXInsightsÎncă nu există evaluări
- 10 Answers To End-Of-Chapter QuestionsDocument10 pagini10 Answers To End-Of-Chapter Questionsalyss ramdathÎncă nu există evaluări
- Holistic Care of People Living With HIV/AIDS by DR A.K. Gupta, DSACSDocument36 paginiHolistic Care of People Living With HIV/AIDS by DR A.K. Gupta, DSACSdr.a.k.gupta6924100% (1)
- SPI RRT Checklist User GuideDocument41 paginiSPI RRT Checklist User GuideUdofia Nicholas100% (1)
- MIND MAPPING OF AIDS IN TERMINAL ILLNESS PATIENTSDocument13 paginiMIND MAPPING OF AIDS IN TERMINAL ILLNESS PATIENTSNamayanja SumayiyahÎncă nu există evaluări
- Factors of Malnutrition in HIV Positive AdolescentsDocument40 paginiFactors of Malnutrition in HIV Positive AdolescentsbagumaÎncă nu există evaluări
- Breastfeeding protects baby and momDocument30 paginiBreastfeeding protects baby and momkholifahnwÎncă nu există evaluări