S-ar putea să vă placă și
- Republic of The PhilippinesDocument1 paginăRepublic of The PhilippinesKezia Magsayo LumasagÎncă nu există evaluări
- Insurance Digested 1Document2 paginiInsurance Digested 1gerlynÎncă nu există evaluări
- Abbot Laboratories v. Alcaraz DigestDocument2 paginiAbbot Laboratories v. Alcaraz DigestEmmanuel Ortega100% (1)
- Be It Enacted by The Senate and House of Representatives of The Philippines in Congress AssembledDocument24 paginiBe It Enacted by The Senate and House of Representatives of The Philippines in Congress AssembledgerlynÎncă nu există evaluări
- Spa FabresDocument2 paginiSpa FabresgerlynÎncă nu există evaluări
- Adolphe Oscar Schuetze's Life Was, by Reason of Its Ownership, Subject To The Inheritance TaxDocument7 paginiAdolphe Oscar Schuetze's Life Was, by Reason of Its Ownership, Subject To The Inheritance TaxgerlynÎncă nu există evaluări
- Interview QuestionsDocument1 paginăInterview QuestionsgerlynÎncă nu există evaluări
- Abbot Laboratories v. Alcaraz DigestDocument2 paginiAbbot Laboratories v. Alcaraz DigestEmmanuel Ortega100% (1)
- AALA vs. UY G.R. No. 202781Document3 paginiAALA vs. UY G.R. No. 202781gerlynÎncă nu există evaluări
- Admin CasesDocument8 paginiAdmin CasesgerlynÎncă nu există evaluări
- Chua Vs CA and Valdes-ChoyDocument2 paginiChua Vs CA and Valdes-ChoygerlynÎncă nu există evaluări
- US v. Pompeya DigestDocument1 paginăUS v. Pompeya DigestArchie Mancol100% (1)
- Magallona Vs ErmitaDocument21 paginiMagallona Vs ErmitaRon GamboaÎncă nu există evaluări
- Sy vs. Gutierrez Robbery Intent To Rob PDFDocument12 paginiSy vs. Gutierrez Robbery Intent To Rob PDFPeterD'Rock WithJason D'ArgonautÎncă nu există evaluări
- Reviewer in Legal Profession and CounsellingDocument8 paginiReviewer in Legal Profession and CounsellingLeo ConsolacionÎncă nu există evaluări
- AALA vs. UY G.R. No. 202781Document3 paginiAALA vs. UY G.R. No. 202781gerlynÎncă nu există evaluări
- Statutory Construction NotesDocument32 paginiStatutory Construction Notespriam gabriel d salidaga95% (102)
- Criminal Law ReviewerDocument262 paginiCriminal Law ReviewerGerry Micor97% (33)
- G.R. No. 122226 March 25, 1998 Mendoza, J:) Will Still Be ExcludedDocument2 paginiG.R. No. 122226 March 25, 1998 Mendoza, J:) Will Still Be ExcludedgerlynÎncă nu există evaluări
- Siquian Vs PeopleDocument1 paginăSiquian Vs PeoplegerlynÎncă nu există evaluări
- Delia Bangalisan Vs CA DigestedDocument1 paginăDelia Bangalisan Vs CA DigestedgerlynÎncă nu există evaluări
- Serafin Vs LindayagDocument1 paginăSerafin Vs LindayaggerlynÎncă nu există evaluări
- People Vs Manuela Flores y SalazarDocument1 paginăPeople Vs Manuela Flores y SalazargerlynÎncă nu există evaluări
- 23 Maligaya STDocument2 pagini23 Maligaya STgerlynÎncă nu există evaluări
- Cruz Vs MijaresDocument1 paginăCruz Vs MijaresgerlynÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Challenges of Financing Small Scale Business Enterprises in NigeriaDocument66 paginiChallenges of Financing Small Scale Business Enterprises in NigeriaShaguolo O. Joseph100% (3)
- Commercial Banking: Pre-Joining AssignmentDocument16 paginiCommercial Banking: Pre-Joining AssignmentsuryanindustriesÎncă nu există evaluări
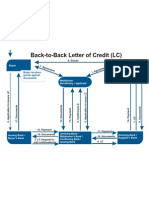
- Back To Back LCDocument1 paginăBack To Back LCJayant Nair0% (1)
- Serfasi ActDocument22 paginiSerfasi ActprakashÎncă nu există evaluări
- Business Loan & Cash Advance Script: (Once The Owner On Phone)Document2 paginiBusiness Loan & Cash Advance Script: (Once The Owner On Phone)Abid RahmanÎncă nu există evaluări
- Part I: Multiple Choices: Choose The Best Answer From The Given Alternatives. (1.5 26 39 PTS.)Document5 paginiPart I: Multiple Choices: Choose The Best Answer From The Given Alternatives. (1.5 26 39 PTS.)solomonaauÎncă nu există evaluări
- Aamra Network LTD Ratio Analysis 2016 2020Document14 paginiAamra Network LTD Ratio Analysis 2016 2020israt jahanÎncă nu există evaluări
- DHFL Sip ReportDocument50 paginiDHFL Sip ReportPragatiÎncă nu există evaluări
- 2022-07 Local 241 NewsletterDocument38 pagini2022-07 Local 241 NewsletterChicago Transit Justice CoalitionÎncă nu există evaluări
- 08-29-2012Document4 pagini08-29-2012gingersnap6Încă nu există evaluări
- Accounting For Managerial DecisionsDocument6 paginiAccounting For Managerial DecisionsKrutika ManeÎncă nu există evaluări
- 2018 Morb PDFDocument1.245 pagini2018 Morb PDFccc jbmÎncă nu există evaluări
- List of Nbfc-Micro Finance Institutions (Nbfc-Mfis) Registered With Rbi (As On January 31, 2022) S No Name of The Company Regional OfficeDocument16 paginiList of Nbfc-Micro Finance Institutions (Nbfc-Mfis) Registered With Rbi (As On January 31, 2022) S No Name of The Company Regional Officepavan yendluriÎncă nu există evaluări
- Students Financial Problems in Higher Education InstitutionsDocument10 paginiStudents Financial Problems in Higher Education InstitutionsAj AbrahamÎncă nu există evaluări
- Letters of Credit-1Document2 paginiLetters of Credit-1Asher RamishÎncă nu există evaluări
- RL05 OriginationDocument42 paginiRL05 Originationvinoth51Încă nu există evaluări
- Project Management MCQ 2Document6 paginiProject Management MCQ 2Muskan SaiyedÎncă nu există evaluări
- 10 18Document128 pagini10 18Woods100% (1)
- Chapter 4. Working Capital ManagementDocument21 paginiChapter 4. Working Capital ManagementHastings Kapala100% (1)
- Arya Financial Services PROPOSAL - OCT - SMCCDocument52 paginiArya Financial Services PROPOSAL - OCT - SMCCSwarna SinghÎncă nu există evaluări
- TỔNG HỢP ĐỀ THI TOEIC READINGDocument49 paginiTỔNG HỢP ĐỀ THI TOEIC READINGmissyou411Încă nu există evaluări
- SanctionDocument2 paginiSanctionBadal Singh Rajput0% (1)
- Interim and Permanent FinancingDocument8 paginiInterim and Permanent FinancingRiya VermaÎncă nu există evaluări
- List of Shelf Companies PDFDocument15 paginiList of Shelf Companies PDFMarshall PeachesÎncă nu există evaluări
- Form 13614-c Intake - Interview Quality Review Sheet 2Document4 paginiForm 13614-c Intake - Interview Quality Review Sheet 2api-593063995Încă nu există evaluări
- Executive Summary:: The Bank of PunjabDocument40 paginiExecutive Summary:: The Bank of PunjabLucifer Morning starÎncă nu există evaluări
- REFI - CMBS 101 - Trepp's Essential Guide To Commercial Mortgage-Backed SecuritiesDocument7 paginiREFI - CMBS 101 - Trepp's Essential Guide To Commercial Mortgage-Backed SecuritiespierrefrancÎncă nu există evaluări
- Working Capital Management PDFDocument46 paginiWorking Capital Management PDFNizar AhamedÎncă nu există evaluări
- New Homes For Sale in Austin, TX by KB HomeDocument1 paginăNew Homes For Sale in Austin, TX by KB HomeNini KikabidzeÎncă nu există evaluări
- Suigeneris: Lecturer: Isaac Christopher L0ubogo (Doctors of Laws Fellow and Doctor of Philosophy Fellow)Document16 paginiSuigeneris: Lecturer: Isaac Christopher L0ubogo (Doctors of Laws Fellow and Doctor of Philosophy Fellow)ochenronaldÎncă nu există evaluări