S-ar putea să vă placă și
- Cantata GuidelinesDocument1 paginăCantata GuidelinesRowel Magsino GonzalesÎncă nu există evaluări
- Chet Atkins Black Mountain Rag1 PDFDocument4 paginiChet Atkins Black Mountain Rag1 PDFDanoBlox100% (1)
- Black Mountain Rag by Chet Atkins PDFDocument4 paginiBlack Mountain Rag by Chet Atkins PDFSantiÎncă nu există evaluări
- CS Form No. 212 Personal Data Sheet RevisedDocument4 paginiCS Form No. 212 Personal Data Sheet RevisedJean Castro76% (106)
- Budget of Work: Computer System Servicing NC IIDocument4 paginiBudget of Work: Computer System Servicing NC IIElmer Oblino Abainza100% (1)
- Biomechanics of The HipDocument12 paginiBiomechanics of The HipSimon Ocares AranguizÎncă nu există evaluări
- DLL MUSIC 8 3rdDocument3 paginiDLL MUSIC 8 3rdRowel Magsino Gonzales100% (7)
- The End of Back Pain: Access Your Hidden Core To Heal Your Body by Patrick Roth, M.D. (Excerpt)Document4 paginiThe End of Back Pain: Access Your Hidden Core To Heal Your Body by Patrick Roth, M.D. (Excerpt)HarperOne (an imprint of HarperCollins)Încă nu există evaluări
- Cost Estimating Manual for Pipelines and Marine Structures: New Printing 1999De la EverandCost Estimating Manual for Pipelines and Marine Structures: New Printing 1999Evaluare: 5 din 5 stele5/5 (2)
- Contrast Media in Diagnostic RadiologyDocument56 paginiContrast Media in Diagnostic RadiologyFaiq Syukri Bin SaparudinÎncă nu există evaluări
- Request For Enrolment With Gap ApprovalDocument2 paginiRequest For Enrolment With Gap ApprovalRowel Magsino Gonzales56% (9)
- Lesson Plan Section IDocument17 paginiLesson Plan Section IAshly NygilÎncă nu există evaluări
- E-Class Record TemplateDocument8 paginiE-Class Record TemplateSaligan DolfÎncă nu există evaluări
- Alveolar OsteitisDocument42 paginiAlveolar OsteitisBastosTemitayoStephen100% (2)
- Technical Livelihood and Education: Quarter 1 - Module 2: Front Office ServicesDocument23 paginiTechnical Livelihood and Education: Quarter 1 - Module 2: Front Office ServicesRowel Magsino Gonzales89% (38)
- Technical Livelihood and Education: Quarter 1 - Module 3: Front Office ServicesDocument28 paginiTechnical Livelihood and Education: Quarter 1 - Module 3: Front Office ServicesRowel Magsino Gonzales100% (7)
- SBIMR Immunization-Forms Rev3Document7 paginiSBIMR Immunization-Forms Rev3Sheryll LezadaÎncă nu există evaluări
- Grade-Sheet - Lessthan75students CTE NEW 1S 22-23Document13 paginiGrade-Sheet - Lessthan75students CTE NEW 1S 22-23judith patnaanÎncă nu există evaluări
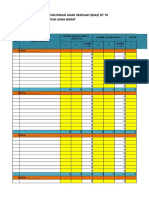
- Form Rekapitulasi Jam Kerja AmanDocument1 paginăForm Rekapitulasi Jam Kerja AmanWahyu Robby PratamaÎncă nu există evaluări
- Produccion Semanal 2024Document43 paginiProduccion Semanal 2024andreamoralermaÎncă nu există evaluări
- Data Rekap Hasil Tes - 2021-2022 TLM Kelas XDocument9 paginiData Rekap Hasil Tes - 2021-2022 TLM Kelas XHaris JuvaÎncă nu există evaluări
- Llmes Qar English Q1-2022-2023Document6 paginiLlmes Qar English Q1-2022-2023Great Zenn RaponÎncă nu există evaluări
- Seal Rotator 8 KDocument16 paginiSeal Rotator 8 Kjonherman220694Încă nu există evaluări
- BI FT Score 2019Document6 paginiBI FT Score 2019Niko MaryadiÎncă nu există evaluări
- Bi FT Score 2019Document6 paginiBi FT Score 2019Niko MaryadiÎncă nu există evaluări
- Jira Hours ReportDocument2 paginiJira Hours ReportOlga RatushniakÎncă nu există evaluări
- Microplanning BIASDocument14 paginiMicroplanning BIASKimya SenandungÎncă nu există evaluări
- Problem Table Algorithm: Company NameDocument1 paginăProblem Table Algorithm: Company NameGloria Elena PerezÎncă nu există evaluări
- Problem Table Algorithm: Company NameDocument1 paginăProblem Table Algorithm: Company NameGiussepi Ali Jhonatan Mamani PacoÎncă nu există evaluări
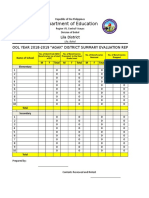
- Department of Education: Lila District School Year 2018-2019 "Agak" District Summary Evaluation ReportDocument1 paginăDepartment of Education: Lila District School Year 2018-2019 "Agak" District Summary Evaluation ReportArnolita Babatuan SolitoÎncă nu există evaluări
- Support Division AFCS Office/Computer Section/Support Staf January 01, 2018 - January 31, 2018 (All Days)Document4 paginiSupport Division AFCS Office/Computer Section/Support Staf January 01, 2018 - January 31, 2018 (All Days)Firis MistludÎncă nu există evaluări
- Tabela Peso Por ÁreaDocument13 paginiTabela Peso Por ÁreaAnderson AndradeÎncă nu există evaluări
- TABLATURA 6, 5 e 4 CORDA-1Document1 paginăTABLATURA 6, 5 e 4 CORDA-1matheuschagas7Încă nu există evaluări
- E-Class Record TemplateDocument72 paginiE-Class Record TemplateJanine Jordan Canlas-BacaniÎncă nu există evaluări
- Inventory Performa GPS Dar Ul Aloom Ghazi AbadDocument26 paginiInventory Performa GPS Dar Ul Aloom Ghazi AbadBilal RashidÎncă nu există evaluări
- Codigos 2021 Imp Todo OfertasDocument218 paginiCodigos 2021 Imp Todo Ofertasjoandi3389Încă nu există evaluări
- E-Class Record TemplateDocument8 paginiE-Class Record TemplateReynan TagabanÎncă nu există evaluări
- Sesnsus Maret 2019Document25 paginiSesnsus Maret 2019ROYALÎncă nu există evaluări
- FrecuenciaDocument2 paginiFrecuenciaCorani Torrez YhoyÎncă nu există evaluări
- TABLATURA 1, 2 e 3 CORDA-1Document1 paginăTABLATURA 1, 2 e 3 CORDA-1matheuschagas7Încă nu există evaluări
- Unix - Time - Start Event Browser - Processed - CountDocument3 paginiUnix - Time - Start Event Browser - Processed - Countganar satoshisÎncă nu există evaluări
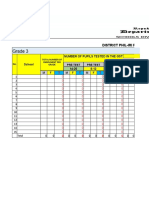
- Phil IRI Forms SY 2021 2022 ElementaryDocument19 paginiPhil IRI Forms SY 2021 2022 ElementaryNenita MendozaÎncă nu există evaluări
- Data Rekap Hasil Tes - SJT TEGALDocument6 paginiData Rekap Hasil Tes - SJT TEGALphewe_goÎncă nu există evaluări
- NO. Name of Institution Province Type of Institution TVI AC: Covid-19 Adjustment Measures Program (Camp) Region VDocument12 paginiNO. Name of Institution Province Type of Institution TVI AC: Covid-19 Adjustment Measures Program (Camp) Region VMyou ChoÎncă nu există evaluări
- Laporan Harian Kegiatan Ori Difteri Bulan Desember 2017 Puskesmas MancakDocument4 paginiLaporan Harian Kegiatan Ori Difteri Bulan Desember 2017 Puskesmas Mancakeyun k firdausÎncă nu există evaluări
- Data Rekap Hasil Tes DAIHATSUDocument7 paginiData Rekap Hasil Tes DAIHATSUNico NicoanÎncă nu există evaluări
- Sma Fransiskus 2 Jakarta Visitors 1678958674451Document17 paginiSma Fransiskus 2 Jakarta Visitors 1678958674451WindymelsÎncă nu există evaluări
- Exogenesis Symphony Part 3 (Redemption)Document1 paginăExogenesis Symphony Part 3 (Redemption)frankÎncă nu există evaluări
- 0-Based Class Record SampleDocument27 pagini0-Based Class Record SampleleonwaypÎncă nu există evaluări
- Lab6 Teste4 Versaoa GrelhaDocument3 paginiLab6 Teste4 Versaoa GrelhaisaÎncă nu există evaluări
- Monthly Product Inventory TemplateDocument3 paginiMonthly Product Inventory TemplateLukas Puguh SantosaÎncă nu există evaluări
- School ID:: Ministry of Basic, Higher and Technical Education (Mbhte)Document21 paginiSchool ID:: Ministry of Basic, Higher and Technical Education (Mbhte)Amrina Acmad100% (1)
- E-Class Spa A 7Document8 paginiE-Class Spa A 7JK De GuzmanÎncă nu există evaluări
- DFBGDocument3 paginiDFBGUnknown_unknown_unknownÎncă nu există evaluări
- Final Debit Note-016Document1 paginăFinal Debit Note-016hhhhhhhuuuuuyyuyyyyyÎncă nu există evaluări
- Control de Inventario MaryfarmaDocument65 paginiControl de Inventario MaryfarmaRossmeryÎncă nu există evaluări
- SAN ISIDRO Report of Rating 2nd QuarterDocument34 paginiSAN ISIDRO Report of Rating 2nd QuarterRizaly PlopenioÎncă nu există evaluări
- Template Bare Individuale - 2013Document677 paginiTemplate Bare Individuale - 2013Emeric ColumbanÎncă nu există evaluări
- Employee Absence TrackingDocument4 paginiEmployee Absence TrackingLea Mae VillanuevaÎncă nu există evaluări
- 01-Planilha+de+Controle+de+Estoque+-+QuantoSobra Com BR+ (FULL)Document1.032 pagini01-Planilha+de+Controle+de+Estoque+-+QuantoSobra Com BR+ (FULL)Marcelo LuizÎncă nu există evaluări
- This White MorningDocument2 paginiThis White MorningMartinÎncă nu există evaluări
- UntitledDocument43 paginiUntitledMaxime AertsÎncă nu există evaluări
- Lab6 Teste3 Versaoa GrelhaDocument3 paginiLab6 Teste3 Versaoa GrelhaisaÎncă nu există evaluări
- 2nd Quarter KPIs SY 2022 2023 Tagongtong ES TemplateDocument94 pagini2nd Quarter KPIs SY 2022 2023 Tagongtong ES TemplateWilma PeñaÎncă nu există evaluări
- Dia Pago Pasaje 8/10/2020 228 5 3 3 5 5 8/11/2020Document3 paginiDia Pago Pasaje 8/10/2020 228 5 3 3 5 5 8/11/2020Julio CruzÎncă nu există evaluări
- SLM Inventory SchoolDocument1.315 paginiSLM Inventory Schoolmarynille joy dela cruzÎncă nu există evaluări
- Pajak TahunanDocument2 paginiPajak Tahunanuftafi viaÎncă nu există evaluări
- Grelha de Correção Da Ficha de Trabalho - Sequência 1. Poesia TrovadorescaDocument2 paginiGrelha de Correção Da Ficha de Trabalho - Sequência 1. Poesia Trovadorescamicla208222Încă nu există evaluări
- Format Kosongan Laporan Harian Pengunaan RDT Antigen Di Faskes Tahun 2021 (1) Dibuatkan Mas Adit File Tambahan KlinikDocument170 paginiFormat Kosongan Laporan Harian Pengunaan RDT Antigen Di Faskes Tahun 2021 (1) Dibuatkan Mas Adit File Tambahan KlinikNIKENÎncă nu există evaluări
- Order and Sales RegisterDocument8 paginiOrder and Sales RegisterchetanÎncă nu există evaluări
- Data Bank VaultDocument12 paginiData Bank Vaulthilmana ilhamÎncă nu există evaluări
- Lab5 Teste 2a GCDocument3 paginiLab5 Teste 2a GCFamília FelizÎncă nu există evaluări
- Advisor Handbook 201320Document48 paginiAdvisor Handbook 201320Rowel Magsino GonzalesÎncă nu există evaluări
- 4th Quarter ADM Module 5 8 Filipino 8 SY 2021 2022 FinalDocument33 pagini4th Quarter ADM Module 5 8 Filipino 8 SY 2021 2022 FinalRowel Magsino Gonzales0% (2)
- 1Document2 pagini1Rowel Magsino GonzalesÎncă nu există evaluări
- Week 1 Q4 ETDocument3 paginiWeek 1 Q4 ETRowel Magsino Gonzales100% (1)
- 04 1 (2) 36 48 PDFDocument13 pagini04 1 (2) 36 48 PDFSushimÎncă nu există evaluări
- HomeworkDocument25 paginiHomeworkapi-260624162Încă nu există evaluări
- Example Univ HandbookDocument161 paginiExample Univ HandbookRowel Magsino GonzalesÎncă nu există evaluări
- Week 1 Q4 ETDocument3 paginiWeek 1 Q4 ETRowel Magsino Gonzales100% (1)
- File Name File Type Modify Date File Size Author Subject Title Page SizeDocument2 paginiFile Name File Type Modify Date File Size Author Subject Title Page SizeRowel Magsino GonzalesÎncă nu există evaluări
- APP Form ADocument2 paginiAPP Form ARowel Magsino GonzalesÎncă nu există evaluări
- Ipcrf 2018 2019 Ti TiiiDocument7 paginiIpcrf 2018 2019 Ti TiiiRowel Magsino GonzalesÎncă nu există evaluări
- Operating System (OS)Document14 paginiOperating System (OS)Rowel Magsino GonzalesÎncă nu există evaluări
- 2015 Saln Form-From CSCDocument3 pagini2015 Saln Form-From CSCRowel Magsino GonzalesÎncă nu există evaluări
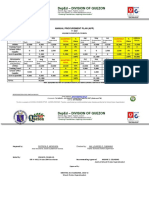
- Deped: Division of QuezonDocument3 paginiDeped: Division of QuezonRowel Magsino GonzalesÎncă nu există evaluări
- DLL MUSIC 8 3rdDocument3 paginiDLL MUSIC 8 3rdRowel Magsino GonzalesÎncă nu există evaluări
- Semi Detailed Lesson Plan in MAPEH For Second YearDocument3 paginiSemi Detailed Lesson Plan in MAPEH For Second Yearien79% (29)
- Gloria Umali Nhs 2019 Mps Per Learning Area 1st To 4th QuarterDocument2 paginiGloria Umali Nhs 2019 Mps Per Learning Area 1st To 4th QuarterRowel Magsino GonzalesÎncă nu există evaluări
- Operating System (OS)Document14 paginiOperating System (OS)Rowel Magsino GonzalesÎncă nu există evaluări
- Math Sir UnadDocument1 paginăMath Sir UnadRowel Magsino GonzalesÎncă nu există evaluări
- MpsDocument2 paginiMpsRowel Magsino GonzalesÎncă nu există evaluări
- Aizel NovelaDocument2 paginiAizel NovelaRowel Magsino GonzalesÎncă nu există evaluări
- ZairaDocument1 paginăZairaRowel Magsino GonzalesÎncă nu există evaluări
- HerniaDocument62 paginiHerniaBen IntosiusÎncă nu există evaluări
- (2365242X - Pharmaceutical Technology in Hospital Pharmacy) Avoid Drug Incompatibilities Clinical Context in Neonatal Intensive Care Unit (NICU)Document8 pagini(2365242X - Pharmaceutical Technology in Hospital Pharmacy) Avoid Drug Incompatibilities Clinical Context in Neonatal Intensive Care Unit (NICU)JoaoÎncă nu există evaluări
- Seattle Children's - Connection Magazine, Fall 2010Document24 paginiSeattle Children's - Connection Magazine, Fall 2010Jeneen CoydanÎncă nu există evaluări
- 2definition of DisasterDocument13 pagini2definition of DisasterRajaÎncă nu există evaluări
- Jadwal Dokter TerbaruDocument1 paginăJadwal Dokter Terbaruphn kitchen idÎncă nu există evaluări
- Growth Comparison in Children With and Without Food Allergies in 2 Different Demographic PopulationsDocument7 paginiGrowth Comparison in Children With and Without Food Allergies in 2 Different Demographic PopulationsMaria Agustina Sulistyo WulandariÎncă nu există evaluări
- Symposium Program - 2017Document16 paginiSymposium Program - 2017api-1937195310% (1)
- Hospital Strategic Plan Presentation ExampleDocument12 paginiHospital Strategic Plan Presentation ExampleDennis DaviesÎncă nu există evaluări
- Pre - & Suffix For HematologyDocument2 paginiPre - & Suffix For HematologyFrieda Cayabyab0% (1)
- 2012 09 Pediatric Report Annex1 2 enDocument187 pagini2012 09 Pediatric Report Annex1 2 enchancechancechanceÎncă nu există evaluări
- Hubungan Penerapan Atraumatic Care Oleh PerawatDocument7 paginiHubungan Penerapan Atraumatic Care Oleh Perawatstrokeunit rsppÎncă nu există evaluări
- No. 27 PDFDocument7 paginiNo. 27 PDFAdilah Zatil KurniaÎncă nu există evaluări
- Biliary AtresiaDocument9 paginiBiliary AtresiaRyrey Abraham PacamanaÎncă nu există evaluări
- 07 17 13Document24 pagini07 17 13grapevineÎncă nu există evaluări
- CGHS HospitalsDocument9 paginiCGHS Hospitalsgarg_mahak3199Încă nu există evaluări
- Catalogue v06Document4 paginiCatalogue v06CxÎncă nu există evaluări
- Phoenix Magazine Top DentistsDocument10 paginiPhoenix Magazine Top DentistspassapgoldyÎncă nu există evaluări
- Blood Transfusion Guidelines 2014Document10 paginiBlood Transfusion Guidelines 2014Trang HuynhÎncă nu există evaluări
- Indria Wahyu Dadang Wibawa - 00000017306Document5 paginiIndria Wahyu Dadang Wibawa - 00000017306Indriano Wahyu Dadang WibawaÎncă nu există evaluări
- Vitreous SubstitutesDocument17 paginiVitreous SubstitutesAnumeha JindalÎncă nu există evaluări
- Case Report Space MaintainerDocument4 paginiCase Report Space MaintainerMufidah NurulÎncă nu există evaluări
- Teorya NG PagtanggapDocument6 paginiTeorya NG PagtanggapMaxine TaeyeonÎncă nu există evaluări
- Infección Urinaria en Niños - NICEDocument31 paginiInfección Urinaria en Niños - NICESu Paola Sanchez DávilaÎncă nu există evaluări
- 7th Edition NRP Brings Big Changes For NRP Instructors: Instructor UpdateDocument12 pagini7th Edition NRP Brings Big Changes For NRP Instructors: Instructor UpdateJoev SaquinÎncă nu există evaluări
- Cells BrochureDocument2 paginiCells Brochureapi-276208942Încă nu există evaluări