S-ar putea să vă placă și
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- HEART FAILURE-WilliamDec (2005) PDFDocument602 paginiHEART FAILURE-WilliamDec (2005) PDFChintya Fidelia MontangÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Efek Statin Dalam Menurunkan Angka Kejadian Penyakit KardiovaskularDocument6 paginiEfek Statin Dalam Menurunkan Angka Kejadian Penyakit KardiovaskularAndrie WigunaÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Tukak GasterDocument11 paginiTukak GasterAndrie WigunaÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- ANEMIA Pada Penyakit KronikDocument14 paginiANEMIA Pada Penyakit KronikAndrie WigunaÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Obesitas Pada Anak: DR - Sri S.Nasar, Spa (K)Document27 paginiObesitas Pada Anak: DR - Sri S.Nasar, Spa (K)Andrie WigunaÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Hershman2018 PDFDocument10 paginiHershman2018 PDFAndrie WigunaÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- PAD Guideline AHA-ACC 2016Document23 paginiPAD Guideline AHA-ACC 2016Andrie WigunaÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Antiplateletdrugs 150203231404 Conversion Gate01 PDFDocument67 paginiAntiplateletdrugs 150203231404 Conversion Gate01 PDFAndrie WigunaÎncă nu există evaluări
- DIVERTIKULOSISDocument28 paginiDIVERTIKULOSISAndrie WigunaÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Nosocomial Pneumonia in AdultsDocument28 paginiNosocomial Pneumonia in AdultsAndrie WigunaÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Plasmodium Malariae Infection in An Asymptomatic 74-Year-OldDocument6 paginiPlasmodium Malariae Infection in An Asymptomatic 74-Year-OldAndrie WigunaÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
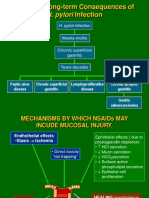
- H. Pylori Infection: Potential Long-Term Consequences ofDocument30 paginiH. Pylori Infection: Potential Long-Term Consequences ofAndrie WigunaÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- NAFLD-dr. Masrul KuliahDocument103 paginiNAFLD-dr. Masrul KuliahAndrie WigunaÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Responding To Organ Failure in HIV-Infected Patients: Volume 348:2279-2281 June 5, 2003 Number 23Document4 paginiResponding To Organ Failure in HIV-Infected Patients: Volume 348:2279-2281 June 5, 2003 Number 23Andrie WigunaÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- H. Pylori Infection: Potential Long-Term Consequences ofDocument30 paginiH. Pylori Infection: Potential Long-Term Consequences ofAndrie WigunaÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- PCR DNA MetodeDocument11 paginiPCR DNA MetodeAndrie WigunaÎncă nu există evaluări
- Executive Summaries of 2000 Updates Anemia Hemodialysis Peritoneal Dialysis Vascular Access Nutrition Chronic Kidney Disease History of DOQIDocument11 paginiExecutive Summaries of 2000 Updates Anemia Hemodialysis Peritoneal Dialysis Vascular Access Nutrition Chronic Kidney Disease History of DOQIAndrie WigunaÎncă nu există evaluări
- Content of The Dossier For Chemical Purity and Microbiological Quality, PA - PH - CEP (04) 1, 6R, December 2018Document16 paginiContent of The Dossier For Chemical Purity and Microbiological Quality, PA - PH - CEP (04) 1, 6R, December 2018Srinivasreddy ChallaÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- A Fire Department Connection CheatsheetDocument5 paginiA Fire Department Connection CheatsheetAhmed HakamÎncă nu există evaluări
- Health Assessment Form For LearnersDocument2 paginiHealth Assessment Form For LearnersIvy Jessa CandilanzaÎncă nu există evaluări
- Liceo de Cagayan University: Bandaging / Applying BandagesDocument5 paginiLiceo de Cagayan University: Bandaging / Applying BandagesTabalbaAcebes GeraldreyÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- SOP - Cleaning of Y-StrainerDocument4 paginiSOP - Cleaning of Y-StrainerKeanu bashÎncă nu există evaluări
- Anti Fog GlassesDocument15 paginiAnti Fog GlassesDanie ChâuÎncă nu există evaluări
- The Mets Direction Our Strategy 2018 2025Document41 paginiThe Mets Direction Our Strategy 2018 2025nobbynobbsÎncă nu există evaluări
- Counselling ReviewerDocument3 paginiCounselling ReviewerEmgee MacmacÎncă nu există evaluări
- HGH SleepDocument6 paginiHGH SleepJibran KhalilÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Kendler InfographicsDocument4 paginiKendler InfographicsMaría Fernanda Ramírez100% (1)
- Maklumat Vaksinasi: Vaccination DetailsDocument2 paginiMaklumat Vaksinasi: Vaccination DetailsAfif HakimÎncă nu există evaluări
- Ascitic Fluid AnalysisDocument3 paginiAscitic Fluid AnalysisLohJÎncă nu există evaluări
- Stability Study of VaccinesDocument13 paginiStability Study of VaccinesHumzaMasoomÎncă nu există evaluări
- Never Try Smoking: ThesisDocument2 paginiNever Try Smoking: ThesisapriramlisÎncă nu există evaluări
- Team Development InterventionsDocument24 paginiTeam Development InterventionsKhushbu Bavishi100% (1)
- Khoiriyyatul Ulfah 181341116Document8 paginiKhoiriyyatul Ulfah 181341116Retno FebriantiÎncă nu există evaluări
- DR - Nasmin.S, MBBS: ObjectiveDocument4 paginiDR - Nasmin.S, MBBS: ObjectiveNasmin AneeshÎncă nu există evaluări
- Psychology Bernstein 9th TBDocument44 paginiPsychology Bernstein 9th TBDevin MckayÎncă nu există evaluări
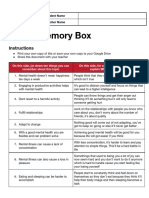
- Mental Health Memory BoxDocument2 paginiMental Health Memory Boxapi-551290426Încă nu există evaluări
- A Cure Is Not WelcomeDocument243 paginiA Cure Is Not WelcomeDesmond AllenÎncă nu există evaluări
- Anabolic SteroidsDocument5 paginiAnabolic SteroidsGideon MurathaÎncă nu există evaluări
- Abraham Maslow's Hierarchy of Needs and Diagrams of Maslow's Motivational TheoryDocument11 paginiAbraham Maslow's Hierarchy of Needs and Diagrams of Maslow's Motivational TheoryHugo MartinsÎncă nu există evaluări
- CRCM 2021 - Final-V2Document136 paginiCRCM 2021 - Final-V2Subra MastroÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- NCP New FormatDocument16 paginiNCP New FormatSophia Marie SoledadÎncă nu există evaluări
- Cambridge Assessment International Education: Biology (Us) 0438/41 October/November 2017Document9 paginiCambridge Assessment International Education: Biology (Us) 0438/41 October/November 2017Mohammad Shahidullah ChowdhuryÎncă nu există evaluări
- Organizational Chart PDFDocument1 paginăOrganizational Chart PDFSabella JimenezÎncă nu există evaluări
- The Mind, The Heart, and The Leader in Times of CrisisDocument16 paginiThe Mind, The Heart, and The Leader in Times of CrisisVeronika BmÎncă nu există evaluări
- BRC Isse 8 Clause 7Document6 paginiBRC Isse 8 Clause 7jacky786Încă nu există evaluări
- Attitudes of Young Adults Towards MarriageDocument12 paginiAttitudes of Young Adults Towards MarriageMehzabin DishaÎncă nu există evaluări
- SK - Cbydp-2020-2022Document21 paginiSK - Cbydp-2020-2022John Joseph TigeroÎncă nu există evaluări
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)De la EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Evaluare: 3 din 5 stele3/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDe la EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDEvaluare: 5 din 5 stele5/5 (2)