S-ar putea să vă placă și
- Wgu Pathophysiology Study Guide d236 Pathophysiology Exam Questions Completed With Correct AnswersDocument12 paginiWgu Pathophysiology Study Guide d236 Pathophysiology Exam Questions Completed With Correct Answersandrew kasaine100% (1)
- Lung Cancer Presentation FinalDocument48 paginiLung Cancer Presentation Finalراس زهد ارفنندÎncă nu există evaluări
- Lifestyle DiseasesDocument44 paginiLifestyle Diseaseskyro draxÎncă nu există evaluări
- Acute Biologic CrisisDocument385 paginiAcute Biologic CrisisSheryl Ann Barit PedinesÎncă nu există evaluări
- Laboratory Diagnosis of Anemia - The Pathophysiology and Types of AnemiaDocument21 paginiLaboratory Diagnosis of Anemia - The Pathophysiology and Types of AnemiaBerfin AlacaÎncă nu există evaluări
- Interpretation of CBCDocument35 paginiInterpretation of CBCnth1992Încă nu există evaluări
- Vasoactive Agents For Adult Septic Shock: An Update and ReviewDocument10 paginiVasoactive Agents For Adult Septic Shock: An Update and ReviewntnquynhproÎncă nu există evaluări
- Drug Therapy of TB, 2015Document44 paginiDrug Therapy of TB, 2015FongChanyipÎncă nu există evaluări
- Severe Lactic Acidosis During Cardiac SurgeryDocument9 paginiSevere Lactic Acidosis During Cardiac SurgeryMarta Quiroz SotoÎncă nu există evaluări
- Stem Cell TransplantationDocument13 paginiStem Cell TransplantationMylls MondejarÎncă nu există evaluări
- A Case of Rectus Sheath HematomaDocument4 paginiA Case of Rectus Sheath HematomadrthirÎncă nu există evaluări
- Antituberculous Therapy in Special SituationsDocument8 paginiAntituberculous Therapy in Special SituationsMobeen Raza100% (1)
- Handbook of Anticancer Pharmacokinetics and Pharmacodynamics 2004Document623 paginiHandbook of Anticancer Pharmacokinetics and Pharmacodynamics 2004Harsh KoshtiÎncă nu există evaluări
- Guidelines For Sedation and Anesthesia in GI Endos PDFDocument11 paginiGuidelines For Sedation and Anesthesia in GI Endos PDFHernan RuedaÎncă nu există evaluări
- Murmur EvaluationDocument4 paginiMurmur EvaluationManjunath GeminiÎncă nu există evaluări
- Nutrition Support in Critically Ill Patients - An Overview - UpToDateDocument23 paginiNutrition Support in Critically Ill Patients - An Overview - UpToDateduong tien truongÎncă nu există evaluări
- CH 46 Complications of AnaesthesiaDocument29 paginiCH 46 Complications of AnaesthesiaChristian LeepoÎncă nu există evaluări
- Drug-Induced QT Interval ProlongationDocument13 paginiDrug-Induced QT Interval ProlongationgeoaislaÎncă nu există evaluări
- Antibiotic Decision Making in IcuDocument11 paginiAntibiotic Decision Making in IcumalvindersahiÎncă nu există evaluări
- Myasthenia Gravis and Other Neuromuscular Junction DisordersDocument8 paginiMyasthenia Gravis and Other Neuromuscular Junction Disordersidno1008Încă nu există evaluări
- Acute Kidney InjuryDocument64 paginiAcute Kidney InjuryBIAN ALKHAZMARIÎncă nu există evaluări
- Acid-Base Tutorial - Kerry BrandisDocument159 paginiAcid-Base Tutorial - Kerry BrandisJason TiongÎncă nu există evaluări
- Pathophysiology 2Document92 paginiPathophysiology 2Princess AgarwalÎncă nu există evaluări
- Chronic Leukemia: Rahmawati Minhajat A. Fachruddin BenyaminDocument24 paginiChronic Leukemia: Rahmawati Minhajat A. Fachruddin BenyaminMJ Putra100% (1)
- Overview of HIV and Its Management: Caroline Mills-Davies Emmanuel FantevieDocument101 paginiOverview of HIV and Its Management: Caroline Mills-Davies Emmanuel FantevieImanuel Fantevie100% (1)
- Oncologic EmergenciesDocument32 paginiOncologic EmergenciesColleen BernilÎncă nu există evaluări
- SARP (Skin Anesthesia Radiology Psychiatry) Review 2010Document4 paginiSARP (Skin Anesthesia Radiology Psychiatry) Review 2010QworldÎncă nu există evaluări
- Why Is A Prothrombin Time Test Performed?: WarfarinDocument6 paginiWhy Is A Prothrombin Time Test Performed?: WarfarinMamta ShindeÎncă nu există evaluări
- BTS Sarcoidosis Clinical StatementDocument17 paginiBTS Sarcoidosis Clinical StatementDarrin WiebeÎncă nu există evaluări
- Module 5A: Dental Management of Patients With Asthma: Prepared By: Dr. Maria Luisa Ramos - ClementeDocument27 paginiModule 5A: Dental Management of Patients With Asthma: Prepared By: Dr. Maria Luisa Ramos - Clementeelaine100% (1)
- Emergency DrugsDocument10 paginiEmergency DrugsnieacatleyaÎncă nu există evaluări
- Sepsis and Septic Shock: Elise Mittleman Boller, - Cynthia M. OttoDocument9 paginiSepsis and Septic Shock: Elise Mittleman Boller, - Cynthia M. OttoIan SabogalÎncă nu există evaluări
- Approach To Septic ShockDocument16 paginiApproach To Septic ShockRaja EllysyaÎncă nu există evaluări
- Hypokalem Ia: Clarisse Cloie Lamberte - BSN3DDocument26 paginiHypokalem Ia: Clarisse Cloie Lamberte - BSN3DClarisse Cloie LamberteÎncă nu există evaluări
- NCCN Guideline RC v3 2022Document20 paginiNCCN Guideline RC v3 2022dony hendrawanÎncă nu există evaluări
- Classification of Anemias: What Is Anemia, How Do You Diagnose Anemia, and How Are The Different Anemias Classified?Document78 paginiClassification of Anemias: What Is Anemia, How Do You Diagnose Anemia, and How Are The Different Anemias Classified?Kaushik BhuvaÎncă nu există evaluări
- Hema II Chapter 7 - BM ExaminationDocument42 paginiHema II Chapter 7 - BM ExaminationKeerthy VasanÎncă nu există evaluări
- Acid Base Equilibrium, Clinical Concepts and Acid Base DisordersDocument64 paginiAcid Base Equilibrium, Clinical Concepts and Acid Base DisordersevanÎncă nu există evaluări
- CANCER History of Cancer Chemotherapy 2008Document12 paginiCANCER History of Cancer Chemotherapy 2008gustavopsoÎncă nu există evaluări
- Max Surgical Blood Order PDFDocument6 paginiMax Surgical Blood Order PDFatina putriÎncă nu există evaluări
- Hypertension SPMDocument25 paginiHypertension SPMSai tejendraÎncă nu există evaluări
- Antiphospholipid Syndrome and Pregnancy (Dengan Foto Punya DR RositaDocument9 paginiAntiphospholipid Syndrome and Pregnancy (Dengan Foto Punya DR RositadidongÎncă nu există evaluări
- Chemotherapy MedicinesDocument2 paginiChemotherapy Medicinesr_mckenrick0% (1)
- Pneumothorax, Tension and TraumaticDocument24 paginiPneumothorax, Tension and TraumaticSatria WibawaÎncă nu există evaluări
- ABG (Arterial Blood Gas Analysis)Document30 paginiABG (Arterial Blood Gas Analysis)kalyan kumarÎncă nu există evaluări
- Complication of Blood TransfusionDocument5 paginiComplication of Blood TransfusionChey Ochy ApriliaÎncă nu există evaluări
- Diagnostic Liver Biopsy PDFDocument7 paginiDiagnostic Liver Biopsy PDFAriadna MarielÎncă nu există evaluări
- Febrile Neutropenia: Nontapak ThiangpakDocument53 paginiFebrile Neutropenia: Nontapak ThiangpakRapid MedicineÎncă nu există evaluări
- Hanson Infectious Diseases - Anamneza I StatusDocument33 paginiHanson Infectious Diseases - Anamneza I StatusSilvia KesegÎncă nu există evaluări
- TizanidineDocument2 paginiTizanidinebhawanisrÎncă nu există evaluări
- Principles of Antibiotics: Deepa V Post Graduate Student DSCDS, BangaloreDocument117 paginiPrinciples of Antibiotics: Deepa V Post Graduate Student DSCDS, BangaloreDeepa VenkateshÎncă nu există evaluări
- Group 2 - ABG INTERPRETATIONDocument2 paginiGroup 2 - ABG INTERPRETATIONJilkiah Mae Alfoja CampomanesÎncă nu există evaluări
- ShockDocument21 paginiShockMin-Joo Esther ParkÎncă nu există evaluări
- Massive Transfusion ProtocolDocument11 paginiMassive Transfusion ProtocolAlaa Abdelmoaty OmranÎncă nu există evaluări
- TLS FinalDocument69 paginiTLS FinalGrace Arthur100% (1)
- BJH Heparin GuidelinesDocument16 paginiBJH Heparin Guidelinesd40sithui100% (1)
- Cancer Risk FactorsDocument44 paginiCancer Risk FactorsSalomo Galih NugrohoÎncă nu există evaluări
- Blood Gas Analysis For Bedside DiagnosisDocument6 paginiBlood Gas Analysis For Bedside DiagnosisMuhamad Wirawan AdityoÎncă nu există evaluări
- Clinical Cheat Sheet: Radiographic AssessmentDocument1 paginăClinical Cheat Sheet: Radiographic AssessmentTracy PopeÎncă nu există evaluări
- Management of Tuberculosis: A guide for clinicians (eBook edition)De la EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Încă nu există evaluări
- National AlcoholDocument63 paginiNational AlcoholMULAT DEGAREGE100% (1)
- Transpo Vrc2010 Tester Manual 2021Document780 paginiTranspo Vrc2010 Tester Manual 2021frederick.lucas4154Încă nu există evaluări
- Official Team Lineups Shakey's V-League Season XDocument10 paginiOfficial Team Lineups Shakey's V-League Season XEli Benjamin Nava TaclinoÎncă nu există evaluări
- DKC Spoilers Arc 1 PDFDocument139 paginiDKC Spoilers Arc 1 PDFdysry100% (4)
- 3 Module in Arts Week 3 4Document8 pagini3 Module in Arts Week 3 4ARVEE DAVE GIPAÎncă nu există evaluări
- OKP For The Preparation of Sodium Hydroxide (0.02 To 1.0 N) & Its Standardization.Document1 paginăOKP For The Preparation of Sodium Hydroxide (0.02 To 1.0 N) & Its Standardization.swapon kumar shillÎncă nu există evaluări
- Nursing Care Plan HydrocephalusDocument7 paginiNursing Care Plan HydrocephalusFarnii MarquezÎncă nu există evaluări
- Lect 6.3 PDFDocument8 paginiLect 6.3 PDFHorlar YeankahÎncă nu există evaluări
- HLR 7965A: Hydraulic Interface ValveDocument2 paginiHLR 7965A: Hydraulic Interface ValveMalique AdamÎncă nu există evaluări
- Indian Botanic Gardens Chapter 4Document16 paginiIndian Botanic Gardens Chapter 4mayank_dwivedi09Încă nu există evaluări
- Tolerance Charting PDFDocument7 paginiTolerance Charting PDFSudeep Kumar SinghÎncă nu există evaluări
- Appendix DatabankDocument4 paginiAppendix DatabankMiriam Torres TorresÎncă nu există evaluări
- 2372 - The Bermuda TriangleDocument97 pagini2372 - The Bermuda TriangleRomain SuchetÎncă nu există evaluări
- Heavy Metals - Environmental Contaminants and Their Occurrence in Different Types of MilkDocument10 paginiHeavy Metals - Environmental Contaminants and Their Occurrence in Different Types of MilkAdeel ZafarÎncă nu există evaluări
- Philippine Navy Enlisted Rating Structure: Military Science (Ms-2)Document10 paginiPhilippine Navy Enlisted Rating Structure: Military Science (Ms-2)Kristine AquitÎncă nu există evaluări
- Numerical Simulation of Interrupted and Conventional Microchannel Heat SinkDocument12 paginiNumerical Simulation of Interrupted and Conventional Microchannel Heat SinkAnkit LonareÎncă nu există evaluări
- RCBC F. AmorsoloDocument16 paginiRCBC F. AmorsoloAyana Mae Baetiong0% (1)
- BendiDocument4 paginiBendicornel_lupuÎncă nu există evaluări
- Fine Group Oy LTD Fine Group Oy LTD Vanha-Littoistentie 2 FI-20660 Littoinen WWW - Finegroup.fiDocument47 paginiFine Group Oy LTD Fine Group Oy LTD Vanha-Littoistentie 2 FI-20660 Littoinen WWW - Finegroup.fitheresadoan100% (1)
- Scope, Objective and Outcome of EEDM (Unit 1)Document27 paginiScope, Objective and Outcome of EEDM (Unit 1)KUSHAL S YADAVÎncă nu există evaluări
- Project Proposal Form (Edexcel) 2Document3 paginiProject Proposal Form (Edexcel) 2Максим КарплюкÎncă nu există evaluări
- PROFIBUS Tester 5 (BC-700-PB) : Mobile Diagnosis of Bus Physics, Communication and CablingDocument3 paginiPROFIBUS Tester 5 (BC-700-PB) : Mobile Diagnosis of Bus Physics, Communication and Cablingchristian villagranÎncă nu există evaluări
- 9 Norms of MoralityDocument34 pagini9 Norms of MoralityDavide LeeÎncă nu există evaluări
- p0420 Catalyst ErrorDocument7 paginip0420 Catalyst Errordion132100% (2)
- ĐỀ THI DỰ ĐOÁN 56 1Document10 paginiĐỀ THI DỰ ĐOÁN 56 1Mai PhạmÎncă nu există evaluări
- Further Readings PDFDocument4 paginiFurther Readings PDFfuad hossainÎncă nu există evaluări
- Arduino Mega 2560 Data SheetDocument23 paginiArduino Mega 2560 Data SheetGodfred NkansahÎncă nu există evaluări
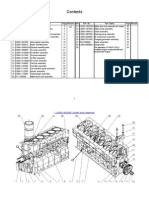
- YC6L 中英文图册Document63 paginiYC6L 中英文图册api-3847557100% (2)
- Mock ExamDocument7 paginiMock ExamJoannaÎncă nu există evaluări
- How To Rent GuideDocument18 paginiHow To Rent Guidechris battleÎncă nu există evaluări