S-ar putea să vă placă și
- Voriconazole Induced PeriostitisDocument4 paginiVoriconazole Induced PeriostitisAsdal AttoÎncă nu există evaluări
- Aging and Cortical Bone Density of Mandible WithDocument5 paginiAging and Cortical Bone Density of Mandible WithAsdal AttoÎncă nu există evaluări
- Aging and Cortical Bone Density of Mandible WithDocument5 paginiAging and Cortical Bone Density of Mandible WithAsdal AttoÎncă nu există evaluări
- Central Giant Cell Granulomaa Case PDFDocument4 paginiCentral Giant Cell Granulomaa Case PDFAsdal AttoÎncă nu există evaluări
- A Rare Tumor of Mediastinum in A Child Giant Mediastinal LipomaDocument3 paginiA Rare Tumor of Mediastinum in A Child Giant Mediastinal LipomaAsdal AttoÎncă nu există evaluări
- Voriconazole Induced PeriostitisDocument4 paginiVoriconazole Induced PeriostitisAsdal AttoÎncă nu există evaluări
- Aging and Cortical Bone Density of Mandible WithDocument5 paginiAging and Cortical Bone Density of Mandible WithAsdal AttoÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- NZ2016SH (32k) - e - NSC5026D 3.3V +100ppmDocument2 paginiNZ2016SH (32k) - e - NSC5026D 3.3V +100ppmDumarronÎncă nu există evaluări
- Company Registration Procedure Handbook in Cambodia, EnglishDocument124 paginiCompany Registration Procedure Handbook in Cambodia, EnglishThea100% (16)
- YhhjjDocument52 paginiYhhjjSam CunananÎncă nu există evaluări
- Alienation Thesis StatementDocument8 paginiAlienation Thesis Statementafbteepof100% (2)
- Bugatti Type 57SCDocument10 paginiBugatti Type 57SCjorge Angel Lope100% (1)
- IEEE 802 StandardsDocument14 paginiIEEE 802 StandardsHoney RamosÎncă nu există evaluări
- PixiiDocument3 paginiPixiiFoxÎncă nu există evaluări
- ADMT Guide: Migrating and Restructuring Active Directory DomainsDocument263 paginiADMT Guide: Migrating and Restructuring Active Directory DomainshtoomaweÎncă nu există evaluări
- Resa Auditing Theorydocx - CompressDocument64 paginiResa Auditing Theorydocx - CompressMaeÎncă nu există evaluări
- Reviewer in EntrepreneurshipDocument6 paginiReviewer in EntrepreneurshipRachelle Anne SaldeÎncă nu există evaluări
- General Characteristics of Phonemes: Aspects of Speech SoundsDocument8 paginiGeneral Characteristics of Phonemes: Aspects of Speech SoundsElina EkimovaÎncă nu există evaluări
- 3 AcmeCorporation Fullstrategicplan 06052015 PDFDocument11 pagini3 AcmeCorporation Fullstrategicplan 06052015 PDFDina DawoodÎncă nu există evaluări
- Microbiological Quality Ice CreamDocument9 paginiMicrobiological Quality Ice CreamocortezlariosÎncă nu există evaluări
- Catalogo Escavadeira EC27CDocument433 paginiCatalogo Escavadeira EC27CNilton Junior Kern50% (2)
- Chapter S1 (Celestial Timekeeping and Navigation)Document28 paginiChapter S1 (Celestial Timekeeping and Navigation)Марко Д. Станковић0% (1)
- Operator'S Manual PM20X-X-X-BXX: 2" Diaphragm PumpDocument12 paginiOperator'S Manual PM20X-X-X-BXX: 2" Diaphragm PumpOmar TadeoÎncă nu există evaluări
- Early Christian ArchitectureDocument38 paginiEarly Christian ArchitectureInspirations & ArchitectureÎncă nu există evaluări
- Ict's - 2022 - Mentorship - Summarized - Thread - by - Trader - Theory - Sep 22, 22 - From - RattibhaDocument11 paginiIct's - 2022 - Mentorship - Summarized - Thread - by - Trader - Theory - Sep 22, 22 - From - RattibhaChristiana OnyinyeÎncă nu există evaluări
- Star Wars Galactic Connexionstm Galactic Beckett Star Wars Story Connexions CallingDocument4 paginiStar Wars Galactic Connexionstm Galactic Beckett Star Wars Story Connexions CallingJuan TorresÎncă nu există evaluări
- Patricio Gerpe ResumeDocument2 paginiPatricio Gerpe ResumeAnonymous 3ID4TBÎncă nu există evaluări
- Alufix Slab Formwork Tim PDFDocument18 paginiAlufix Slab Formwork Tim PDFMae FalcunitinÎncă nu există evaluări
- Weekly Lesson Plan: Pry 3 (8years) Third Term Week 1Document12 paginiWeekly Lesson Plan: Pry 3 (8years) Third Term Week 1Kunbi Santos-ArinzeÎncă nu există evaluări
- Altos Easystore Users ManualDocument169 paginiAltos Easystore Users ManualSebÎncă nu există evaluări
- Crusader Castle Al-Karak Jordan Levant Pagan Fulk, King of Jerusalem MoabDocument3 paginiCrusader Castle Al-Karak Jordan Levant Pagan Fulk, King of Jerusalem MoabErika CalistroÎncă nu există evaluări
- Listening Tests 81112Document13 paginiListening Tests 81112luprof tpÎncă nu există evaluări
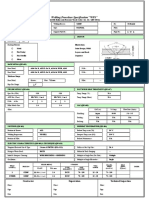
- Wps For Carbon Steel THK 7.11 GtawDocument1 paginăWps For Carbon Steel THK 7.11 GtawAli MoosaviÎncă nu există evaluări
- HC+ Shoring System ScaffoldDocument31 paginiHC+ Shoring System ScaffoldShafiqÎncă nu există evaluări
- MikoritkDocument6 paginiMikoritkChris Jonathan Showip RouteÎncă nu există evaluări
- Science Grade 10 (Exam Prep)Document6 paginiScience Grade 10 (Exam Prep)Venice Solver100% (3)
- Sheet (8) Synchronous Machine Problem (1) :: SolutionDocument5 paginiSheet (8) Synchronous Machine Problem (1) :: Solutionمكاريوس عيادÎncă nu există evaluări