S-ar putea să vă placă și
- Mump EmedicineDocument15 paginiMump Emedicinekeyla_shineeeÎncă nu există evaluări
- Chapter 9: MeaslesDocument16 paginiChapter 9: MeaslesTrixie Marie Sabile AbdullaÎncă nu există evaluări
- Measles: Questions and Answers: Information About The Disease and VaccinesDocument4 paginiMeasles: Questions and Answers: Information About The Disease and VaccinesIles Reen Chan AlvarezÎncă nu există evaluări
- Selected References: Mumps Vaccines Studies On Immune Responses, Efficacy and EffectivenessDocument11 paginiSelected References: Mumps Vaccines Studies On Immune Responses, Efficacy and EffectivenessekowahyudiÎncă nu există evaluări
- Tambahan TransleteDocument9 paginiTambahan TransleteRamadhana PutraÎncă nu există evaluări
- Levy Mwanawasa Medical University School of Public Health and Environmental Sciences Department of Public HealthDocument5 paginiLevy Mwanawasa Medical University School of Public Health and Environmental Sciences Department of Public HealthChristían KanyataÎncă nu există evaluări
- Epidemiology of Measles in The Philippines: Original ArticleDocument10 paginiEpidemiology of Measles in The Philippines: Original ArticlePearlÎncă nu există evaluări
- Duration of Immunit of MeaslesDocument8 paginiDuration of Immunit of MeaslesBakolonÎncă nu există evaluări
- Annotated BibliographyDocument19 paginiAnnotated Bibliographyapi-455648185Încă nu există evaluări
- Measles:: Questions and AnswersDocument4 paginiMeasles:: Questions and AnswersAustine OsaweÎncă nu există evaluări
- Mumps StudyDocument10 paginiMumps StudyNational Content DeskÎncă nu există evaluări
- Deeks MumpsDocument7 paginiDeeks Mumpsj wONGÎncă nu există evaluări
- Mumps Virus Vaccines: WHO Position PaperDocument9 paginiMumps Virus Vaccines: WHO Position PaperMaya HalimÎncă nu există evaluări
- Measles, Mumps, Rubella (MMR) Vaccine Discussion Pack: An Information Guide For Health Professionals and ParentsDocument9 paginiMeasles, Mumps, Rubella (MMR) Vaccine Discussion Pack: An Information Guide For Health Professionals and Parentsscribd-123Încă nu există evaluări
- 189 Supplement - 1 s116Document7 pagini189 Supplement - 1 s116Eliska NÎncă nu există evaluări
- Questions and Answers: MumpsDocument4 paginiQuestions and Answers: MumpsHannahÎncă nu există evaluări
- Campak AnakDocument17 paginiCampak AnakFaskanita NadapdapÎncă nu există evaluări
- Am J Epidemiol - 2000-Dourado-524-30Document7 paginiAm J Epidemiol - 2000-Dourado-524-30api-246003035Încă nu există evaluări
- Introducing Combined Measles, Mumps and Rubella Vaccine in Chandigarh, India: Issues and Concerns!Document3 paginiIntroducing Combined Measles, Mumps and Rubella Vaccine in Chandigarh, India: Issues and Concerns!wiweksharmaÎncă nu există evaluări
- Measles - Vaccine Preventable Diseases Surveillance Manual CDCDocument20 paginiMeasles - Vaccine Preventable Diseases Surveillance Manual CDCRetno ViraÎncă nu există evaluări
- Introducing Combined Measles, Mumps and Rubella Vaccine in Chandigarh, India: Issues and Concerns!Document3 paginiIntroducing Combined Measles, Mumps and Rubella Vaccine in Chandigarh, India: Issues and Concerns!Muhammad Aalam KhanÎncă nu există evaluări
- Mumps in Pulaski CountyDocument2 paginiMumps in Pulaski CountyC.J. GardnerÎncă nu există evaluări
- MeaslesDocument4 paginiMeaslesChandan KonwarÎncă nu există evaluări
- MMR Poster 1Document1 paginăMMR Poster 1Grace WongÎncă nu există evaluări
- Vaksin VarelaDocument8 paginiVaksin VarelaPutra EkaÎncă nu există evaluări
- NVACJAMA Measles EpidemicDocument7 paginiNVACJAMA Measles EpidemicjmdagingÎncă nu există evaluări
- Virus Paramyxovirus: MorbillivirusDocument9 paginiVirus Paramyxovirus: MorbillivirusRhoda Mae Dano JandayanÎncă nu există evaluări
- J.22-09-2011 VaricellaDocument3 paginiJ.22-09-2011 VaricellaIndra PolenkÎncă nu există evaluări
- Measles and Rubella: Learning A Lesson The Hard WayDocument2 paginiMeasles and Rubella: Learning A Lesson The Hard WayMarilyn GonzalesÎncă nu există evaluări
- Piis0025619619305737 220530 065558Document11 paginiPiis0025619619305737 220530 065558Garcia Yepez Stephanie GraceÎncă nu există evaluări
- 1297.full Mahasiswa Kedokteran UmumDocument4 pagini1297.full Mahasiswa Kedokteran UmumArya KusumaÎncă nu există evaluări
- Mumps Vaccine Performance Among University Students During A Mumps OutbreakDocument9 paginiMumps Vaccine Performance Among University Students During A Mumps OutbreakNopita Speed3Încă nu există evaluări
- Pediatrics 2012 Klein 809 14Document8 paginiPediatrics 2012 Klein 809 14Myrtle SetiawanÎncă nu există evaluări
- Journal 1Document8 paginiJournal 1DICKY DEWANTOROÎncă nu există evaluări
- Varicella Post-ProphylaxisDocument2 paginiVaricella Post-ProphylaxisAngelaTrinidadÎncă nu există evaluări
- MMR 2 Vaccine InsertDocument11 paginiMMR 2 Vaccine InsertJonÎncă nu există evaluări
- Investigating The Cases of Measles Among Children Under 5 Years Old in Abu Ali Sina Balkhi Education Seminary HospitalDocument5 paginiInvestigating The Cases of Measles Among Children Under 5 Years Old in Abu Ali Sina Balkhi Education Seminary HospitalInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Chapter 17: Varicella: I. Disease DescriptionDocument17 paginiChapter 17: Varicella: I. Disease DescriptionMihaiLÎncă nu există evaluări
- What Are The Symptoms Measles (Focus On Measles More, Then Talk About Mumps and Rubella)Document2 paginiWhat Are The Symptoms Measles (Focus On Measles More, Then Talk About Mumps and Rubella)RexDavidGidoÎncă nu există evaluări
- Epidemiol Rev 2006 Robinson 81 7Document7 paginiEpidemiol Rev 2006 Robinson 81 7chie_8866Încă nu există evaluări
- Vaccines Cause Autism.: TH TH THDocument3 paginiVaccines Cause Autism.: TH TH THWannadiebuttoscared KillÎncă nu există evaluări
- Measles: Protecting Children From Measles With The MMR VaccinationDocument10 paginiMeasles: Protecting Children From Measles With The MMR VaccinationAfra FitrianitaÎncă nu există evaluări
- Badanie MMRDocument8 paginiBadanie MMRAgaryÎncă nu există evaluări
- Prevention and Treatment of Seasonal Influenza: Clinical PracticeDocument7 paginiPrevention and Treatment of Seasonal Influenza: Clinical PracticeDias PradikaÎncă nu există evaluări
- Prophylactic Antipyretics For Prevention of Febrile Seizures Following VaccinationDocument3 paginiProphylactic Antipyretics For Prevention of Febrile Seizures Following VaccinationEddie WyattÎncă nu există evaluări
- Perspectives: Misleading Media Reporting? The MMR StoryDocument6 paginiPerspectives: Misleading Media Reporting? The MMR StoryGurgehÎncă nu există evaluări
- Cancer HBO-BMLDocument3 paginiCancer HBO-BMLThumiso MasohaÎncă nu există evaluări
- Mumps Public FaqDocument9 paginiMumps Public FaqMckerwinÎncă nu există evaluări
- If Maglalagay Kayo Info. Separate Niyo Narin Yung Ilalagay Sa PPT Na Mga Keywords para Di Na Mahirapan MamayaDocument11 paginiIf Maglalagay Kayo Info. Separate Niyo Narin Yung Ilalagay Sa PPT Na Mga Keywords para Di Na Mahirapan MamayaJhay-r BaldoÎncă nu există evaluări
- (R) Varicella VirusDocument8 pagini(R) Varicella VirusEkkim Al KindiÎncă nu există evaluări
- Lecture 2 - MeaslesDocument33 paginiLecture 2 - MeaslesShaimaa AbdulkadirÎncă nu există evaluări
- Chaturvedi 1998Document4 paginiChaturvedi 1998NorashidaHassanÎncă nu există evaluări
- E MumpsDocument3 paginiE Mumpsolivia1026Încă nu există evaluări
- Trop Med Int Health 2009 - p167Document7 paginiTrop Med Int Health 2009 - p167Astri Faluna SheylavontiaÎncă nu există evaluări
- Estimation of Vaccine Efficacy and Critical Vaccination Coverage in Partially Observed OutbreaksDocument9 paginiEstimation of Vaccine Efficacy and Critical Vaccination Coverage in Partially Observed OutbreaksAri SiswadiÎncă nu există evaluări
- Journal Reading Angelo Alexander 1522321040Document5 paginiJournal Reading Angelo Alexander 1522321040Muhammad ulhaqÎncă nu există evaluări
- J School Nurs 2012 - p9-12Document4 paginiJ School Nurs 2012 - p9-12Astri Faluna SheylavontiaÎncă nu există evaluări
- Effectiveness of A Third Dose of MMR Vaccine For Mumps Outbreak ControlDocument10 paginiEffectiveness of A Third Dose of MMR Vaccine For Mumps Outbreak ControlMuhammad FachrurozieÎncă nu există evaluări
- DynamedDocument41 paginiDynamedkaren AlvaradoÎncă nu există evaluări
- Chronic Dry Cough in Allergic Respiratory Diseases: Diagnostic and Management ApproachDocument6 paginiChronic Dry Cough in Allergic Respiratory Diseases: Diagnostic and Management ApproachAaron HongreiÎncă nu există evaluări
- Account Statement From 1 Apr 2019 To 30 Apr 2019: TXN Date Value Date Description Ref No./Cheque No. Debit Credit BalanceDocument2 paginiAccount Statement From 1 Apr 2019 To 30 Apr 2019: TXN Date Value Date Description Ref No./Cheque No. Debit Credit BalanceAaron HongreiÎncă nu există evaluări
- PcytDocument8 paginiPcytAaron HongreiÎncă nu există evaluări
- Edoc - Pub Nms InstallationDocument1 paginăEdoc - Pub Nms InstallationAaron HongreiÎncă nu există evaluări
- BB LFMT AppConfiguration VideoCalling 17042018Document10 paginiBB LFMT AppConfiguration VideoCalling 17042018Aaron HongreiÎncă nu există evaluări
- .. Link Analysis Report: Site InformationDocument3 pagini.. Link Analysis Report: Site InformationAaron HongreiÎncă nu există evaluări
- RS-232 Port Leds USB Port: Product OverviewDocument2 paginiRS-232 Port Leds USB Port: Product OverviewAaron HongreiÎncă nu există evaluări
- Configuring IEEE 802.1Q TunnelingDocument8 paginiConfiguring IEEE 802.1Q TunnelingAaron HongreiÎncă nu există evaluări
- Corrigendum Regarding Holding of LICE JTODocument4 paginiCorrigendum Regarding Holding of LICE JTOAaron HongreiÎncă nu există evaluări
- Huaweifp2255 Ifwt ServiceDocument1 paginăHuaweifp2255 Ifwt ServiceAaron HongreiÎncă nu există evaluări
- C) SL - No.1491 To SL - No.1500 10 NosDocument1 paginăC) SL - No.1491 To SL - No.1500 10 NosAaron HongreiÎncă nu există evaluări
- Manual IPasolink 200Document58 paginiManual IPasolink 200Aaron HongreiÎncă nu există evaluări
- Element Manager User Guide Release 2.3.0: Part Number: 10-00116-02-A0Document176 paginiElement Manager User Guide Release 2.3.0: Part Number: 10-00116-02-A0Aaron HongreiÎncă nu există evaluări
- 01 SOP For CRM Clarity User Side System Settings PDFDocument11 pagini01 SOP For CRM Clarity User Side System Settings PDFAaron Hongrei0% (1)
- Gujarat Telecom Circle: Ahmedabad Broadband Equipment Preventive Maintenance ManualDocument55 paginiGujarat Telecom Circle: Ahmedabad Broadband Equipment Preventive Maintenance ManualAaron Hongrei0% (1)
- Frequency BandsDocument6 paginiFrequency BandsAaron HongreiÎncă nu există evaluări
- Herpes PresentationDocument10 paginiHerpes PresentationOkafor AugustineÎncă nu există evaluări
- Herpes Opportunity Disclosure Handout 2Document1 paginăHerpes Opportunity Disclosure Handout 2Thong Huynh100% (1)
- PCR 1 - Nashita Nawal Dzikra. NNDocument1 paginăPCR 1 - Nashita Nawal Dzikra. NNDesy Ariza Eka PutriÎncă nu există evaluări
- Sample VOID : Certificate of ImmunizationDocument2 paginiSample VOID : Certificate of ImmunizationYou Can never guessÎncă nu există evaluări
- Measles PamphletDocument2 paginiMeasles PamphletDom DomÎncă nu există evaluări
- Paramyxoviruses: Dr. Muna M A Yousif M.D Clinical MicrobiologyDocument30 paginiParamyxoviruses: Dr. Muna M A Yousif M.D Clinical MicrobiologyJaydee PlataÎncă nu există evaluări
- Biro Administrasi Dan Akademik (Baak) : Berita Acara Kegiatan Belajar Mengajar (KBM)Document3 paginiBiro Administrasi Dan Akademik (Baak) : Berita Acara Kegiatan Belajar Mengajar (KBM)Juventus HuruleanÎncă nu există evaluări
- Chickenpox (Varicella) : What Is Chickenpox? What Are The Symptoms of Chickenpox?Document3 paginiChickenpox (Varicella) : What Is Chickenpox? What Are The Symptoms of Chickenpox?Helga Yoan Ladymeyer TimbayoÎncă nu există evaluări
- CDC Hiv Pep101Document2 paginiCDC Hiv Pep101Sangeetha HospitalÎncă nu există evaluări
- 5 Facts Poster - Easy Read 2021Document6 pagini5 Facts Poster - Easy Read 2021Olek NowakÎncă nu există evaluări
- S2 Curs 5 - Infectii Virale. ExantemDocument63 paginiS2 Curs 5 - Infectii Virale. ExantemRegele BrânzăÎncă nu există evaluări
- INFEKSI HIV DAN HSV PADA OBSTETRI GINEKOLOGI - DR - Edi Wibowo A, SP - OG (K)Document24 paginiINFEKSI HIV DAN HSV PADA OBSTETRI GINEKOLOGI - DR - Edi Wibowo A, SP - OG (K)Rahayu AyuÎncă nu există evaluări
- Enveloped and Non Enveloped VirusDocument10 paginiEnveloped and Non Enveloped ViruspixholicÎncă nu există evaluări
- The Varicella-Zoster Virus Vaccines - Benefit and RisksDocument17 paginiThe Varicella-Zoster Virus Vaccines - Benefit and RisksermaendahÎncă nu există evaluări
- Hand Foot and Mouth Disease Fact SheetDocument3 paginiHand Foot and Mouth Disease Fact SheetBreixo HarguindeyÎncă nu există evaluări
- HIV Awareness BrochureDocument2 paginiHIV Awareness BrochureLoraine Antonette CupoÎncă nu există evaluări
- What Are The Symptoms Measles (Focus On Measles More, Then Talk About Mumps and Rubella)Document2 paginiWhat Are The Symptoms Measles (Focus On Measles More, Then Talk About Mumps and Rubella)RexDavidGidoÎncă nu există evaluări
- Prevalence of Hepatitis B and C Virus Infection Among Pregnant Women With HIV/AIDS Attending Antenatal Clinic in Health Facilities in FCT: A Retrospective StudyDocument5 paginiPrevalence of Hepatitis B and C Virus Infection Among Pregnant Women With HIV/AIDS Attending Antenatal Clinic in Health Facilities in FCT: A Retrospective StudyInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Virology Influenza Nad ParainfluenzaDocument4 paginiVirology Influenza Nad ParainfluenzaHisham ChomanyÎncă nu există evaluări
- Dr. Bernice E. Eddy Cutter VaccineDocument1 paginăDr. Bernice E. Eddy Cutter VaccineCTSoldierÎncă nu există evaluări
- Shingles RecombinantDocument2 paginiShingles Recombinantn99aliÎncă nu există evaluări
- Reportable DiseasesDocument1 paginăReportable DiseasescrcespÎncă nu există evaluări
- Faktor Lingkungan Sosial, Lingkungan Fisik, Dan Pengendalian Program DBD Terhadap Kejadian Demam Berdarah Dengue (DBD)Document6 paginiFaktor Lingkungan Sosial, Lingkungan Fisik, Dan Pengendalian Program DBD Terhadap Kejadian Demam Berdarah Dengue (DBD)Azat GoblinÎncă nu există evaluări
- Philippine Star, Jan. 20, 2020, House To Probe Return of Polio PDFDocument1 paginăPhilippine Star, Jan. 20, 2020, House To Probe Return of Polio PDFpribhor2Încă nu există evaluări
- List of PPAS To Combat Acquired Immune Deficiency SyndromeDocument4 paginiList of PPAS To Combat Acquired Immune Deficiency SyndromeLeonard ArenasÎncă nu există evaluări
- Triptico Del EbolaDocument2 paginiTriptico Del EbolaClaudi TperezÎncă nu există evaluări
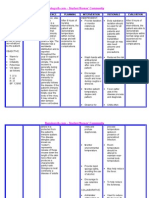
- NURSING CARE PLAN Chicken PoxDocument2 paginiNURSING CARE PLAN Chicken Poxderic87% (62)
- Pulse Polio Days 20th June, 2010 To 24th June, 2010Document4 paginiPulse Polio Days 20th June, 2010 To 24th June, 2010Amey DhatrakÎncă nu există evaluări
- Power Point On Chicken PoxDocument9 paginiPower Point On Chicken PoxSpongebobGGG100% (1)
- ExcelDocument2 paginiExcelNur YahmanÎncă nu există evaluări