S-ar putea să vă placă și
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingDe la EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingÎncă nu există evaluări
- Inflammatory Colitis - A RecapDocument34 paginiInflammatory Colitis - A RecapanahitaasharmaÎncă nu există evaluări
- Skin Soft Tissue Infections 1 - 27 - 2019Document14 paginiSkin Soft Tissue Infections 1 - 27 - 2019Muhammad Azhar ImranÎncă nu există evaluări
- Diagnosis Treatment and Prevention of Typhoid Fever in Adults 2017Document11 paginiDiagnosis Treatment and Prevention of Typhoid Fever in Adults 2017Khayla Ray RondobioÎncă nu există evaluări
- IBD Surgical AlgorithmDocument30 paginiIBD Surgical AlgorithmKarthik SubramaniamÎncă nu există evaluări
- DIARRHEADocument12 paginiDIARRHEAtintin srgpnÎncă nu există evaluări
- MSA in STIDocument36 paginiMSA in STISuhazeli Abdullah100% (2)
- Orthopaedic Infection in Adults UHL GuidelineDocument10 paginiOrthopaedic Infection in Adults UHL GuidelineFadlu ManafÎncă nu există evaluări
- Acute Abdominal Pain Pathway: Management - Primary Care and Community SettingsDocument2 paginiAcute Abdominal Pain Pathway: Management - Primary Care and Community Settingsshella1selinaÎncă nu există evaluări
- UTI Treatment Algorithm - Sharp Mesa Vista 2Document3 paginiUTI Treatment Algorithm - Sharp Mesa Vista 2Fitri 1997Încă nu există evaluări
- UTI TreatmentDocument3 paginiUTI TreatmentMaria RezitadinaÎncă nu există evaluări
- Bowels Open 6 Times Per 24 Hours: Document ControlDocument7 paginiBowels Open 6 Times Per 24 Hours: Document ControlKeith PohlÎncă nu există evaluări
- Management of Sexually Transmitted Diseases and Hiv AidsDocument28 paginiManagement of Sexually Transmitted Diseases and Hiv AidsUtkarsh YadavÎncă nu există evaluări
- Drug Study NicoleDocument6 paginiDrug Study NicoleFrancheska Nicole Delos SantosÎncă nu există evaluări
- Tetanus Immune Globulin (TIG) : IndicationsDocument5 paginiTetanus Immune Globulin (TIG) : IndicationsShams JailaniÎncă nu există evaluări
- Antibiotic Guidelines For BONE AND JOINT INFECTIONSDocument3 paginiAntibiotic Guidelines For BONE AND JOINT INFECTIONSKhurram NadeemÎncă nu există evaluări
- Shivani PDFDocument3 paginiShivani PDFdeepukumarÎncă nu există evaluări
- Vince Drug Study LaboratoryDocument6 paginiVince Drug Study LaboratoryUzziel Galinea TolosaÎncă nu există evaluări
- (2009) Gout PDFDocument11 pagini(2009) Gout PDFWilsonne ChuaÎncă nu există evaluări
- Needle Stick InjuryDocument9 paginiNeedle Stick Injuryinfectioncontrol department100% (1)
- Handbook of Sexual DysfunctionDocument1 paginăHandbook of Sexual DysfunctionRenato SánchezÎncă nu există evaluări
- G JaundiceDocument40 paginiG JaundiceRedina Tuya RamirezÎncă nu există evaluări
- Leptospirosis ReviewDocument3 paginiLeptospirosis ReviewKathrina AbastarÎncă nu există evaluări
- OmeprazoleDocument2 paginiOmeprazoleIvan Matthew SuperioÎncă nu există evaluări
- Museum IDocument37 paginiMuseum ISirish KunwarÎncă nu există evaluări
- Management of Infection in Primary Care Adapted For Local UseDocument15 paginiManagement of Infection in Primary Care Adapted For Local UseWizri SuharianiÎncă nu există evaluări
- 4 NCP-Impaired Skin IntegrityDocument3 pagini4 NCP-Impaired Skin IntegrityMhil Ishan Margate100% (1)
- Antibiotic-Associated Diarrhea: Quick Recertific Ation SeriesDocument2 paginiAntibiotic-Associated Diarrhea: Quick Recertific Ation SeriesDeril RidwanÎncă nu există evaluări
- Stemi ChecklistDocument1 paginăStemi ChecklistDanu SusantoÎncă nu există evaluări
- Guidelines Ut I 2012Document1 paginăGuidelines Ut I 2012Siti ZulaikhahÎncă nu există evaluări
- NCP - 3B - Naila Ferdia Putri1130019059 - Uts Bahasa Inggris.Document7 paginiNCP - 3B - Naila Ferdia Putri1130019059 - Uts Bahasa Inggris.Nayla FerdianaÎncă nu există evaluări
- A. Background of The StudyDocument43 paginiA. Background of The StudyJohn Robert CruzÎncă nu există evaluări
- Dr. Wahyuni Indawati, Spa (K)Document43 paginiDr. Wahyuni Indawati, Spa (K)Rara AnisaÎncă nu există evaluări
- Pal EarningsDocument107 paginiPal EarningsSarah Ong SiuÎncă nu există evaluări
- Burns GuidelineDocument1 paginăBurns GuidelineRoi LevinzonÎncă nu există evaluări
- Intestnal ObstructionDocument4 paginiIntestnal ObstructionRenea Joy ArruejoÎncă nu există evaluări
- Management of Nonperforated Appendicitis in AdultsDocument1 paginăManagement of Nonperforated Appendicitis in Adultsjoaoduarte95Încă nu există evaluări
- Monkeypox Protocol - V1.0 (2047833421)Document5 paginiMonkeypox Protocol - V1.0 (2047833421)Syed AhmedÎncă nu există evaluări
- Answers, Rationales, and Test Taking Strategies: 4. It Is Important For The Nurse To RecognizeDocument10 paginiAnswers, Rationales, and Test Taking Strategies: 4. It Is Important For The Nurse To RecognizeNursyNurseÎncă nu există evaluări
- Soal Ujian Perawat Teladan ADocument25 paginiSoal Ujian Perawat Teladan AMutmainna MakmurÎncă nu există evaluări
- Ceftriaxone SodiumDocument2 paginiCeftriaxone SodiumSTORAGE FILEÎncă nu există evaluări
- Corneal Disease and Dystrophy Management PDFDocument53 paginiCorneal Disease and Dystrophy Management PDFScerbatiuc CristinaÎncă nu există evaluări
- Preventing Opioid-Induced ConstipationDocument2 paginiPreventing Opioid-Induced Constipationaib reisÎncă nu există evaluări
- 7 Cases FungalDocument56 pagini7 Cases Fungalkoteshwara raoÎncă nu există evaluări
- rd-15 Bartholin Cyst and Abscess 10-12 PDFDocument2 paginird-15 Bartholin Cyst and Abscess 10-12 PDFdevidanthonyÎncă nu există evaluări
- Hirschsprung Disease Clinical Guideline: in Both Preoperative and Postoperative For Many Years After SurgeryDocument3 paginiHirschsprung Disease Clinical Guideline: in Both Preoperative and Postoperative For Many Years After SurgeryRudyard Paul AmistadÎncă nu există evaluări
- Nursing Training NABHDocument11 paginiNursing Training NABHVisali RathinakumarÎncă nu există evaluări
- Brajac - ProtocolDocument13 paginiBrajac - Protocolthanh ngôÎncă nu există evaluări
- Algorithms For IV Fluid The RapyDocument1 paginăAlgorithms For IV Fluid The RapyEdwinÎncă nu există evaluări
- Jurding Anak PolriDocument41 paginiJurding Anak PolriRizkyaFarhanÎncă nu există evaluări
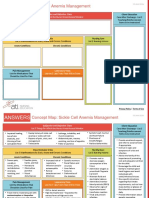
- NCC-SickleCellAnemiaManagement ConceptMap InteractivePDFDocument2 paginiNCC-SickleCellAnemiaManagement ConceptMap InteractivePDFLoggerz Arck100% (1)
- GNR Bacteremia De-Escalation Guide Final PDFDocument2 paginiGNR Bacteremia De-Escalation Guide Final PDFAbu Hammoud AlyazeediÎncă nu există evaluări
- PromDocument33 paginiPromkisÎncă nu există evaluări
- Adhesive Intestinal Obstruction. What A Resident Should KnowDocument6 paginiAdhesive Intestinal Obstruction. What A Resident Should Knowrahul ranjanÎncă nu există evaluări
- How Much Do We Know About Constipation After Surgery For Anorectal Malformation?Document5 paginiHow Much Do We Know About Constipation After Surgery For Anorectal Malformation?Ade Triansyah EmsilÎncă nu există evaluări
- Polypharmacy: Guidance For Prescribing in Frail AdultsDocument6 paginiPolypharmacy: Guidance For Prescribing in Frail AdultsAgil BredlyÎncă nu există evaluări
- Dur Sun 2019Document4 paginiDur Sun 2019Dayane GonçalvesÎncă nu există evaluări
- Case Study of UTIDocument6 paginiCase Study of UTIAmina TariqÎncă nu există evaluări
- HydroceleDocument10 paginiHydroceleRyan ReÎncă nu există evaluări
- De La Cruz, A - BSN 3b - Case Study For RM 219 - 1st Week of DutyDocument13 paginiDe La Cruz, A - BSN 3b - Case Study For RM 219 - 1st Week of DutyAlia De La CruzÎncă nu există evaluări
- Islamic Architecture PDFDocument59 paginiIslamic Architecture PDFHarshi Garg100% (3)
- Kumpulan Soal UPDocument16 paginiKumpulan Soal UPTriono SusantoÎncă nu există evaluări
- Different Varieties of English C1 WSDocument5 paginiDifferent Varieties of English C1 WSLaurie WÎncă nu există evaluări
- Farewell Address WorksheetDocument3 paginiFarewell Address Worksheetapi-261464658Încă nu există evaluări
- Cases Torts 7-29-17 DigestDocument1 paginăCases Torts 7-29-17 Digestczabina fatima delicaÎncă nu există evaluări
- Missions ETC 2020 SchemesOfWarDocument10 paginiMissions ETC 2020 SchemesOfWarDanieleBisignanoÎncă nu există evaluări
- Friday Night Mishaps, Listening Plus TasksDocument3 paginiFriday Night Mishaps, Listening Plus TasksCristina Stoian100% (1)
- Italian CuisineDocument29 paginiItalian CuisinekresnayandraÎncă nu există evaluări
- Case DigestsDocument12 paginiCase DigestsHusni B. SaripÎncă nu există evaluări
- Homeless Class ActionDocument36 paginiHomeless Class ActionMichael_Lee_RobertsÎncă nu există evaluări
- 03 Dizon v. COMELECDocument1 pagină03 Dizon v. COMELECChelle BelenzoÎncă nu există evaluări
- Savage Cyberpunk 2020Document14 paginiSavage Cyberpunk 2020dmage_uÎncă nu există evaluări
- The Fat Cat Called PatDocument12 paginiThe Fat Cat Called PatAlex ArroÎncă nu există evaluări
- Math - Gr6 - Q2 - Week-08 - Comparing and Arranging Integers On The Number LineDocument37 paginiMath - Gr6 - Q2 - Week-08 - Comparing and Arranging Integers On The Number LineDiana TubigÎncă nu există evaluări
- Apollo Hospital Chennai: NO: 16, BSNL TELESHOPPE, Greams Road 044 2999 1606Document9 paginiApollo Hospital Chennai: NO: 16, BSNL TELESHOPPE, Greams Road 044 2999 1606Manas ChandaÎncă nu există evaluări
- Online Book Store System: Bachelor of Computer EngineeringDocument31 paginiOnline Book Store System: Bachelor of Computer Engineeringkalpesh mayekarÎncă nu există evaluări
- Notice: List of Eligible Candidate(s)Document3 paginiNotice: List of Eligible Candidate(s)Ram KumarÎncă nu există evaluări
- Region 2Document75 paginiRegion 2yoyiyyiiyiyÎncă nu există evaluări
- College Physics Global 10th Edition Young Solutions ManualDocument25 paginiCollege Physics Global 10th Edition Young Solutions ManualSaraSmithdgyj100% (57)
- Aci - The Financial Markets Association: Examination FormulaeDocument8 paginiAci - The Financial Markets Association: Examination FormulaeJovan SsenkandwaÎncă nu există evaluări
- Business Communication and Behavioural StudiesDocument10 paginiBusiness Communication and Behavioural StudiesBhujangam NaiduÎncă nu există evaluări
- Pechay Camote Buchi - Aug7Document36 paginiPechay Camote Buchi - Aug7Rockie Alibio JuanicoÎncă nu există evaluări
- Doanh Nghiep Viet Nam Quang CaoDocument1 paginăDoanh Nghiep Viet Nam Quang Caodoanhnghiep100% (1)
- Eastwoods: College of Science and Technology, IncDocument2 paginiEastwoods: College of Science and Technology, IncMichael AustriaÎncă nu există evaluări
- Students' Rights: Atty. Mabelyn A. Palukpok Commission On Human Rights-CarDocument15 paginiStudents' Rights: Atty. Mabelyn A. Palukpok Commission On Human Rights-Cardhuno teeÎncă nu există evaluări
- How To Install Linux, Apache, MySQL, PHP (LAMP) Stack On Ubuntu 16.04Document12 paginiHow To Install Linux, Apache, MySQL, PHP (LAMP) Stack On Ubuntu 16.04Rajesh kÎncă nu există evaluări
- Bhrighu Saral Paddhati - 1Document212 paginiBhrighu Saral Paddhati - 1ErrovioÎncă nu există evaluări
- Artikel Andi Nurindah SariDocument14 paginiArtikel Andi Nurindah Sariapril yansenÎncă nu există evaluări
- Human Computer Interaction LECTURE 1Document19 paginiHuman Computer Interaction LECTURE 1mariya ali100% (2)