S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Taxation As A Major Source of Govt. FundingDocument47 paginiTaxation As A Major Source of Govt. FundingPriyali Rai50% (2)
- Lessons From The TrailDocument12 paginiLessons From The TrailNeel Kashkari50% (2)
- 1505727274wpdm - Regulamentul ANCPIDocument340 pagini1505727274wpdm - Regulamentul ANCPIValentina TurcuÎncă nu există evaluări
- The Great Moving Nowhere Show (Hall, 1998)Document6 paginiThe Great Moving Nowhere Show (Hall, 1998)GiorgosÎncă nu există evaluări
- Personal HygieneDocument23 paginiPersonal Hygieneksraghavan2000Încă nu există evaluări
- 6 - Elements SummaryDocument17 pagini6 - Elements Summaryksraghavan2000Încă nu există evaluări
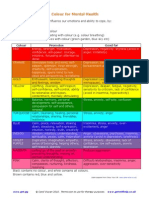
- ColourBreathing PDFDocument2 paginiColourBreathing PDFCabinet Psihoterapie Camelia DemeterÎncă nu există evaluări
- List of Tamil SongsDocument8 paginiList of Tamil Songsksraghavan2000Încă nu există evaluări
- Song ListDocument180 paginiSong Listksraghavan2000Încă nu există evaluări
- Song ListDocument180 paginiSong Listksraghavan2000Încă nu există evaluări
- Justin Davenport - Teacher Retention in The United StatesDocument19 paginiJustin Davenport - Teacher Retention in The United Statesapi-310209692Încă nu există evaluări
- Capitalism Kritik GenericsDocument43 paginiCapitalism Kritik GenericsZakCherifÎncă nu există evaluări
- Innovation and Inclusive GrowthDocument7 paginiInnovation and Inclusive Growthjeny babuÎncă nu există evaluări
- The K To 12 Basic Education Program ARTICLESDocument65 paginiThe K To 12 Basic Education Program ARTICLESCarla Joyce89% (18)
- Labour's 50 Top AchievementsDocument2 paginiLabour's 50 Top AchievementsSan SharmaÎncă nu există evaluări
- What Is SBMDocument34 paginiWhat Is SBMjyzgnzls21Încă nu există evaluări
- Female Education PDFDocument4 paginiFemale Education PDFSalma JanÎncă nu există evaluări
- 04 CDP 2017 2020Document21 pagini04 CDP 2017 2020Chesca LaurinÎncă nu există evaluări
- The Impact of Global Capitalism On Economic Development in NigeriaDocument67 paginiThe Impact of Global Capitalism On Economic Development in NigeriaTomiloba Olaniyi-quadriÎncă nu există evaluări
- Exxon Drilling in GuyanaDocument15 paginiExxon Drilling in GuyanaAdeel TabassumÎncă nu există evaluări
- Thesis SampleDocument60 paginiThesis SampleJessamin SantanderÎncă nu există evaluări
- Honest Accounts 2017 - How The World Profits From Africa's WealthDocument12 paginiHonest Accounts 2017 - How The World Profits From Africa's WealthJoao SoaresÎncă nu există evaluări
- Position PaperDocument7 paginiPosition PaperJohn Angelo O. De La CruzÎncă nu există evaluări
- Annotated BibliographyDocument4 paginiAnnotated Bibliographyapi-317220035Încă nu există evaluări
- PFM Reform Strategy 2016-21 FinalDocument104 paginiPFM Reform Strategy 2016-21 FinalShafiqulHasanÎncă nu există evaluări
- Pierre Bourdieu and Abdelmalek SayadDocument43 paginiPierre Bourdieu and Abdelmalek SayadGabi Maas100% (1)
- Lesson 2: Gender and Development Awareness: 2. Definition of TermsDocument13 paginiLesson 2: Gender and Development Awareness: 2. Definition of TermsBaucas, Rolanda D.Încă nu există evaluări
- If The Idea Like Marshall Plan Is Implemented in Many Poor African Countries, This World Would Be A Better PlaceDocument2 paginiIf The Idea Like Marshall Plan Is Implemented in Many Poor African Countries, This World Would Be A Better PlaceFeliantika WijayantiÎncă nu există evaluări
- Housing Group 5 Paper Revision Sa Analysis DapitDocument21 paginiHousing Group 5 Paper Revision Sa Analysis DapitDenise GorgolonÎncă nu există evaluări
- Domestic Water Consumption Pattern by Urban HousehDocument12 paginiDomestic Water Consumption Pattern by Urban HousehBla3Încă nu există evaluări
- Artica, Sandy Mae, D. SOCSCI 1105 BSAC 3-1 1 Sem. A.Y. 2020-2021Document4 paginiArtica, Sandy Mae, D. SOCSCI 1105 BSAC 3-1 1 Sem. A.Y. 2020-2021SandyÎncă nu există evaluări
- NAT Reviewer Critical ThinkingDocument20 paginiNAT Reviewer Critical ThinkingMaria Eleonor C. Bañares100% (2)
- VCD Guide PDFDocument31 paginiVCD Guide PDFMohammad Sameed ZaheerÎncă nu există evaluări
- The Winds of Change: Climate Change, Poverty and The Environment in MalawiDocument52 paginiThe Winds of Change: Climate Change, Poverty and The Environment in MalawiOxfamÎncă nu există evaluări
- Children of The Market - Comment Is Free - Guardian - Co.ukDocument26 paginiChildren of The Market - Comment Is Free - Guardian - Co.ukjulienrharrisonÎncă nu există evaluări
- Imbong V Hon. Ochoa, Jr. GR NO. 204819 APRIL 8, 2014 FactsDocument8 paginiImbong V Hon. Ochoa, Jr. GR NO. 204819 APRIL 8, 2014 FactsJack NumosÎncă nu există evaluări