S-ar putea să vă placă și
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Bleeding Time, Clotting Time PT and PTT2Document41 paginiBleeding Time, Clotting Time PT and PTT2Qurrataini Ibanez100% (1)
- Medicosis Perfectionalis Clinical Vignettes Bleeding (FREE SAMPLE)Document7 paginiMedicosis Perfectionalis Clinical Vignettes Bleeding (FREE SAMPLE)Rocky Bhai100% (1)
- Hemostasis ReviewerDocument14 paginiHemostasis ReviewerDayledaniel SorvetoÎncă nu există evaluări
- DIC PathophysiologyDocument1 paginăDIC Pathophysiologykathy100% (1)
- Bleeding DisordersDocument24 paginiBleeding Disorderskholoud220Încă nu există evaluări
- Course Outline Hematology 2Document4 paginiCourse Outline Hematology 2Nichole SilverioÎncă nu există evaluări
- Disseminated Intravascular CoagulationDocument19 paginiDisseminated Intravascular CoagulationAnna MilliziaÎncă nu există evaluări
- Inserto Tiempo de TrombinaDocument3 paginiInserto Tiempo de TrombinaAnonymous 34YMghpÎncă nu există evaluări
- Coagularea Intravasculara DiseminataDocument6 paginiCoagularea Intravasculara DiseminataAlex Ungureanu100% (2)
- PT & aPTTDocument3 paginiPT & aPTTWho KnowsÎncă nu există evaluări
- Experiment 11: Bleeding Disorder Excessive Clotting Disorder AnticoagulantDocument3 paginiExperiment 11: Bleeding Disorder Excessive Clotting Disorder AnticoagulantDhyu FernaÎncă nu există evaluări
- Receipt of Sample: HUSM/HEMA - UPT/QP - 01Document10 paginiReceipt of Sample: HUSM/HEMA - UPT/QP - 01zakwanmustafaÎncă nu există evaluări
- Secondary Clotting DisordersDocument34 paginiSecondary Clotting DisordersLyra Dennise LlidoÎncă nu există evaluări
- Platelet Von Willebrand Factor in Hermansky-Pudlak Syndrome (American Journal of Hematology, Vol. 59, Issue 2) (1998)Document6 paginiPlatelet Von Willebrand Factor in Hermansky-Pudlak Syndrome (American Journal of Hematology, Vol. 59, Issue 2) (1998)Ahmed MagzoubÎncă nu există evaluări
- SIEMENS - Thromborel SDocument8 paginiSIEMENS - Thromborel Senrique santillanÎncă nu există evaluări
- Secondary HemostasisDocument24 paginiSecondary Hemostasisalibayaty1Încă nu există evaluări
- Acquired Coagulation DisordersDocument11 paginiAcquired Coagulation DisordersAli AhmedÎncă nu există evaluări
- Learning ObjectivesDocument12 paginiLearning ObjectivesjmcvicenteÎncă nu există evaluări
- Hypercoagulable State & Anticoagulant Therapy: Dr. Kamal E. HiggyDocument22 paginiHypercoagulable State & Anticoagulant Therapy: Dr. Kamal E. HiggyAndrew StorerÎncă nu există evaluări
- PLT MeasurementsDocument6 paginiPLT MeasurementsAudreySlitÎncă nu există evaluări
- Jurnal 1. Koagulasi Dan Golongan DarahDocument8 paginiJurnal 1. Koagulasi Dan Golongan DarahnisrinaÎncă nu există evaluări
- Bleeding DisordersDocument10 paginiBleeding Disorderslyli Star AngeloÎncă nu există evaluări
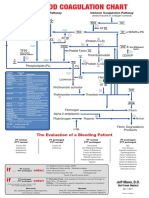
- Blood Clotting ChartDocument1 paginăBlood Clotting ChartBianca SimionescuÎncă nu există evaluări
- Coagulation Pathway and Physiology: Jerry B. Lefkowitz, MDDocument10 paginiCoagulation Pathway and Physiology: Jerry B. Lefkowitz, MDdilaÎncă nu există evaluări
- Art Deco AssignmentDocument20 paginiArt Deco AssignmentAmerÎncă nu există evaluări
- SEED No 1 - COAG - Principles of HaemostasisDocument4 paginiSEED No 1 - COAG - Principles of HaemostasisM Yusuf Ali RÎncă nu există evaluări
- Disseminated Intravascular Coagulation (DIC) During Pregnancy - Clinical Findings, Etiology, and Diagnosis - UpToDateDocument23 paginiDisseminated Intravascular Coagulation (DIC) During Pregnancy - Clinical Findings, Etiology, and Diagnosis - UpToDateCristinaCaprosÎncă nu există evaluări
- Anticoagulant Anti Platelet Fibrinolytic Drugs08 Black and WhiteDocument28 paginiAnticoagulant Anti Platelet Fibrinolytic Drugs08 Black and WhiteJagdesh SajnaniÎncă nu există evaluări
- Protein C DeficiencyDocument6 paginiProtein C DeficiencyDimas Rio BaltiÎncă nu există evaluări
- Mechanism of Blood Clotting Extensic Pathway Factors Affecting Blood ClottingDocument18 paginiMechanism of Blood Clotting Extensic Pathway Factors Affecting Blood ClottingRaunak TripathiÎncă nu există evaluări