S-ar putea să vă placă și
- Hoffman S 2018Document14 paginiHoffman S 2018Putry SampelanÎncă nu există evaluări
- Status Trauma PDFDocument12 paginiStatus Trauma PDFLee EunHye LimÎncă nu există evaluări
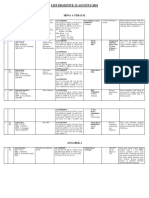
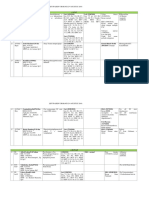
- 15 Agustus 2018 List A Teratai UpdatedDocument2 pagini15 Agustus 2018 List A Teratai UpdatedLee EunHye LimÎncă nu există evaluări
- DocumentDocument4 paginiDocumentLee EunHye LimÎncă nu există evaluări
- Status Non Trauma PDFDocument8 paginiStatus Non Trauma PDFLee EunHye LimÎncă nu există evaluări
- Teratai + Luar 19.08.2018Document2 paginiTeratai + Luar 19.08.2018Lee EunHye LimÎncă nu există evaluări
- Status Non Trauma PDFDocument8 paginiStatus Non Trauma PDFLee EunHye LimÎncă nu există evaluări
- Teratai + Luar 19.08.2018Document2 paginiTeratai + Luar 19.08.2018Lee EunHye LimÎncă nu există evaluări
- 04/08/2018 (Klinik Patra) : A TerataiDocument3 pagini04/08/2018 (Klinik Patra) : A TerataiLee EunHye LimÎncă nu există evaluări
- Konsensus HipertiroidDocument6 paginiKonsensus HipertiroidDiethaKusumaningrumÎncă nu există evaluări
- Daftar Hadir Health EducationDocument2 paginiDaftar Hadir Health EducationLee EunHye LimÎncă nu există evaluări
- Pap Smear Brochure PDFDocument2 paginiPap Smear Brochure PDFLee EunHye LimÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Acute Liver FailureDocument13 paginiAcute Liver FailureDiana YvetteÎncă nu există evaluări
- Physician Certification FormDocument2 paginiPhysician Certification FormSachin Tukaram SalianÎncă nu există evaluări
- Pediatric Meds List1Document38 paginiPediatric Meds List1Arman Carl DulayÎncă nu există evaluări
- Chronic Interstitial (Restrictive Infiltrative) Lung DiseasesDocument44 paginiChronic Interstitial (Restrictive Infiltrative) Lung DiseasesAntony WaithakaÎncă nu există evaluări
- Efektivitas Penggunaan Media Video Learning Multimedia (VLM) Terhadap Pengetahuan Infeksi Menular Seksual (Ims) (Studi Pada Waria Di Kota Makassar)Document6 paginiEfektivitas Penggunaan Media Video Learning Multimedia (VLM) Terhadap Pengetahuan Infeksi Menular Seksual (Ims) (Studi Pada Waria Di Kota Makassar)Muhammad Fajrul Falah KholifaturrahmanÎncă nu există evaluări
- Gastroenteritis Case ReportDocument12 paginiGastroenteritis Case ReportjisooÎncă nu există evaluări
- Functional analysis of episodic self-injury linked to ear infectionsDocument3 paginiFunctional analysis of episodic self-injury linked to ear infectionsTimiÎncă nu există evaluări
- Vaccination and Autoimmune Disease: What Is The Evidence?: ReviewDocument8 paginiVaccination and Autoimmune Disease: What Is The Evidence?: Reviewtito7227Încă nu există evaluări
- MeningococcemiaDocument15 paginiMeningococcemiaJoma CabiLdo ﭢÎncă nu există evaluări
- Prevent Malaria in PregnancyDocument18 paginiPrevent Malaria in PregnancyHamza Dawid HamidÎncă nu există evaluări
- 2019 Evaluation and Management of The Febrile Young Infant in The Emergency DepartmentDocument31 pagini2019 Evaluation and Management of The Febrile Young Infant in The Emergency DepartmentMonica ValderramaÎncă nu există evaluări
- How Changes in Body Weight Affect GERDDocument3 paginiHow Changes in Body Weight Affect GERDIce BibovskiÎncă nu există evaluări
- Granuloma Inguinale 2Document32 paginiGranuloma Inguinale 2Elsa MayoraÎncă nu există evaluări
- Jurnal MalabsorbsiDocument6 paginiJurnal MalabsorbsiIda Putri IhsaniÎncă nu există evaluări
- Fever Without A Source in The 1 - To 3-Month-Old Infant Case FileDocument2 paginiFever Without A Source in The 1 - To 3-Month-Old Infant Case Filehttps://medical-phd.blogspot.comÎncă nu există evaluări
- Ards Case StudyDocument1 paginăArds Case StudyLyons MacÎncă nu există evaluări
- VET PREVENTIVE MEDICINE EXAMDocument8 paginiVET PREVENTIVE MEDICINE EXAMashish kumarÎncă nu există evaluări
- Schizoaffective Disorder FactsheetDocument16 paginiSchizoaffective Disorder FactsheetVictoria AdhityaÎncă nu există evaluări
- Tumours of The OvaryDocument36 paginiTumours of The OvaryZahidul ZahidÎncă nu există evaluări
- Lecture 8 - SCI 8007SEF Medical Microbiology & Virology-Virology II - 2023Document76 paginiLecture 8 - SCI 8007SEF Medical Microbiology & Virology-Virology II - 2023YY CheungÎncă nu există evaluări
- Communicable Disease NursingDocument23 paginiCommunicable Disease NursingWinter SparkleÎncă nu există evaluări
- Omphalitis LectureDocument18 paginiOmphalitis LectureWonyenghitari George0% (1)
- Antibiotic Guidelines For AdultsDocument9 paginiAntibiotic Guidelines For AdultsVarshini Tamil SelvanÎncă nu există evaluări
- Symptoms of Chronic Liver DiseaseDocument5 paginiSymptoms of Chronic Liver DiseaseAhmed HassanÎncă nu există evaluări
- Guidelines for Health Workers on the Thai-Myanmar BorderDocument322 paginiGuidelines for Health Workers on the Thai-Myanmar BorderAhmed MubarakÎncă nu există evaluări
- Covid19 Banerji ProtocolDocument3 paginiCovid19 Banerji ProtocolAga Kiermasz100% (4)
- Module 4.4 NotesDocument5 paginiModule 4.4 Notesa2a4alensunnyÎncă nu există evaluări
- BC COMPLICATIONS & PROGNOSISDocument42 paginiBC COMPLICATIONS & PROGNOSISalalmaee1Încă nu există evaluări
- Berylliosis Definition and CausesDocument13 paginiBerylliosis Definition and Causesrahaf qatawnehÎncă nu există evaluări
- Iman Ismanto 06031985Document1 paginăIman Ismanto 06031985Deni MalikÎncă nu există evaluări