S-ar putea să vă placă și
- Caderneta19 VacinacaoDocument2 paginiCaderneta19 VacinacaoAna Lopes80% (5)
- Cartão de Vacina CriançaDocument2 paginiCartão de Vacina CriançaClaudia Araújo73% (11)
- Caderneta FinalDocument31 paginiCaderneta FinalrpoiÎncă nu există evaluări
- 2022 Modelo Cartão Sombra Da CriançaDocument2 pagini2022 Modelo Cartão Sombra Da CriançatiagoÎncă nu există evaluări
- Cartão de VacinçãoDocument7 paginiCartão de VacinçãoCatia Ribeiro da SilvaÎncă nu există evaluări
- Ficha Registro Vacinado1 SIPNI PDFDocument2 paginiFicha Registro Vacinado1 SIPNI PDFRone LimaÎncă nu există evaluări
- Cartão Da Criança 2021 Caderneta de VacinasDocument2 paginiCartão Da Criança 2021 Caderneta de VacinasIngrid RodriguesÎncă nu există evaluări
- Cartão de Vacina AdultoDocument2 paginiCartão de Vacina AdultoClaudia Araújo100% (1)
- Ficha de Registro Do VacinadoDocument2 paginiFicha de Registro Do Vacinadoflimas100% (5)
- Cronograma de EstudosDocument6 paginiCronograma de EstudosLayane Fernandes100% (1)
- Enfermagem Note - 28.02Document18 paginiEnfermagem Note - 28.02Denise Silva44% (9)
- Modelo Laudo Ecg PDFDocument1 paginăModelo Laudo Ecg PDFCassi Avlis Cent67% (3)
- Guia de Bolso Calculo Da DPP e IgDocument1 paginăGuia de Bolso Calculo Da DPP e IgexuperiofariasÎncă nu există evaluări
- Avaliação FinalDocument6 paginiAvaliação FinalLuan Gomes50% (4)
- Caderno de Estagio 2021 - 1 PDFDocument41 paginiCaderno de Estagio 2021 - 1 PDFLeonardo SantosÎncă nu există evaluări
- Ficha Registro Acompanhamento Vacinado 2018Document2 paginiFicha Registro Acompanhamento Vacinado 2018Paulo MatiasÎncă nu există evaluări
- SMS007 Requisicao de Exames ComplementaresDocument2 paginiSMS007 Requisicao de Exames ComplementaresDeyvison FerreiraÎncă nu există evaluări
- JMS - IMP.1761.01 - Ficha de Admissão Colaborador - Não ClínicosDocument5 paginiJMS - IMP.1761.01 - Ficha de Admissão Colaborador - Não ClínicosFilipa AdriãoÎncă nu există evaluări
- Agência Nacional de Vigilância SanitáriaDocument4 paginiAgência Nacional de Vigilância Sanitáriajulia osorioÎncă nu există evaluări
- Requisicao ColpoDocument1 paginăRequisicao Colpokleberson arrudaÎncă nu există evaluări
- Formulario Requisicao Resultado Exame Histopatologico Colo UteroDocument2 paginiFormulario Requisicao Resultado Exame Histopatologico Colo UteroThiago Ferreira100% (1)
- Ficha DomalbertoDocument1 paginăFicha DomalbertoPedro AugustoÎncă nu există evaluări
- Ficha Anamnese1 PDFDocument1 paginăFicha Anamnese1 PDFKhaos LcfÎncă nu există evaluări
- Modelo Histrico Escolar Ensino Fundamental A Partir de 2020Document16 paginiModelo Histrico Escolar Ensino Fundamental A Partir de 2020Matheus SilvaÎncă nu există evaluări
- Requisicao de Exame Histopatologico11072008Document2 paginiRequisicao de Exame Histopatologico11072008Fabiana SantosÎncă nu există evaluări
- Formulário para Requisições de Exames - Citopatológico (Mama) 416Document2 paginiFormulário para Requisições de Exames - Citopatológico (Mama) 416VenusLa0% (1)
- Laudo Médico de Tratamento Fora Do Domicílio (LM)Document6 paginiLaudo Médico de Tratamento Fora Do Domicílio (LM)tatiana miranda costaÎncă nu există evaluări
- Ficha-de-Inscricao-Fut 2023Document1 paginăFicha-de-Inscricao-Fut 2023Fut CumbucoÎncă nu există evaluări
- Ficha de Matrícula Uniabeu 2021 PósDocument1 paginăFicha de Matrícula Uniabeu 2021 PósAline BarbosaÎncă nu există evaluări
- Ficha de Cadastro Admissional - CLTDocument2 paginiFicha de Cadastro Admissional - CLTLucas GodoiÎncă nu există evaluări
- Caderno de Estatísticas Do Programa VIH-SIDA 02.10.2018Document12 paginiCaderno de Estatísticas Do Programa VIH-SIDA 02.10.2018claudiomsamba20Încă nu există evaluări
- Formulario para Requisicoes de Exames - Mamografia 332 PDFDocument2 paginiFormulario para Requisicoes de Exames - Mamografia 332 PDFRafael Luciano100% (1)
- Sistema de Gerenciamento de ClubesDocument1 paginăSistema de Gerenciamento de ClubesNathália Sousa PintoÎncă nu există evaluări
- INSCRIÇÃO DE GRUPO SCFV 2021 - CópiaDocument2 paginiINSCRIÇÃO DE GRUPO SCFV 2021 - CópiaCRAS Geralda MedeirosÎncă nu există evaluări
- Requisicao de Exames Complementares 2017Document2 paginiRequisicao de Exames Complementares 2017alceufjrÎncă nu există evaluări
- Guia Encam Cadaver 2013Document3 paginiGuia Encam Cadaver 2013Manuela Oliveira MarinhoÎncă nu există evaluări
- Formulario para Requisicoes Mamografia (Com Destaques)Document2 paginiFormulario para Requisicoes Mamografia (Com Destaques)Gabriel Rocha100% (2)
- Ficha de Vacinação Covid Trabalhadores EducaçaoDocument1 paginăFicha de Vacinação Covid Trabalhadores EducaçaoMaria Da silvaÎncă nu există evaluări
- Carteira Nacional de Vacinação DigitalDocument1 paginăCarteira Nacional de Vacinação Digitalnatasha celiraÎncă nu există evaluări
- Hist Escolar EF - A Partir de 2020 - V2Document20 paginiHist Escolar EF - A Partir de 2020 - V2maria victóriaÎncă nu există evaluări
- 04 - Ficha de Cadastro e Termo - Recebimento de Novos Membros e CongregadosDocument1 pagină04 - Ficha de Cadastro e Termo - Recebimento de Novos Membros e CongregadosEliza MariaÎncă nu există evaluări
- Ministério Da Saúde Requisição de Exame Citopatológico - MamaDocument2 paginiMinistério Da Saúde Requisição de Exame Citopatológico - MamaLETICIA ROSANE CRUZÎncă nu există evaluări
- Requisicao de Exames Complementares 2017Document2 paginiRequisicao de Exames Complementares 2017Rainer LopesÎncă nu există evaluări
- Hist Escolar EF - 2021Document1 paginăHist Escolar EF - 2021Hans GrudzinskiÎncă nu există evaluări
- Edital 2022 0000001Document10 paginiEdital 2022 0000001Daniela Sant'anaÎncă nu există evaluări
- Hist Escolar EM - A Partir de 2020 - V2Document19 paginiHist Escolar EM - A Partir de 2020 - V2elmar eustaquioÎncă nu există evaluări
- Ficha de Matrícula Fac 2021 PósDocument1 paginăFicha de Matrícula Fac 2021 PósLuis Felipe Figueiredo de OliveiraÎncă nu există evaluări
- Requisição de Exame Laboratorial para Diagnóstico de RaivaDocument1 paginăRequisição de Exame Laboratorial para Diagnóstico de RaivaMateus AlbaÎncă nu există evaluări
- NRE - Anexo X Termo de Compromisso de NAO Estágio ObrigatórioDocument8 paginiNRE - Anexo X Termo de Compromisso de NAO Estágio Obrigatórion.jacksonÎncă nu există evaluări
- Ilovepdf MergedDocument22 paginiIlovepdf MergedMarcos AndréÎncă nu există evaluări
- Ficha de MatriculaDocument1 paginăFicha de MatriculaRadio CamaquenseÎncă nu există evaluări
- Anexo 5 - Formulário B - SocioeconômicoDocument4 paginiAnexo 5 - Formulário B - SocioeconômicolauroÎncă nu există evaluări
- Ficha de Matrícula Faveni 2021 PósDocument1 paginăFicha de Matrícula Faveni 2021 PósLázaro SilvaÎncă nu există evaluări
- Ficha Professor AcademiaDocument2 paginiFicha Professor AcademiaMatheus PereiraÎncă nu există evaluări
- Atualização de Dados Modelo SISAP CTCDocument1 paginăAtualização de Dados Modelo SISAP CTCThiago SantosÎncă nu există evaluări
- Hist Escolar EF - 2021Document28 paginiHist Escolar EF - 2021Hans GrudzinskiÎncă nu există evaluări
- Aee Diario de Classe Individual mppb2018Document54 paginiAee Diario de Classe Individual mppb2018Patrícia Novaes100% (2)
- Protocolo de Vacinação Antirrábica Pré-ExposiçãoDocument2 paginiProtocolo de Vacinação Antirrábica Pré-ExposiçãoMilena Camara100% (1)
- D Formulario-Socioeconomico 2023 Fct-VeteranosDocument9 paginiD Formulario-Socioeconomico 2023 Fct-VeteranosPedro PiinÎncă nu există evaluări
- Ficha Cadastro de Cliente SebraeDocument1 paginăFicha Cadastro de Cliente SebraeMarcos SouzaÎncă nu există evaluări
- Ambiente Nas Organizações e Turbulência Ambiental - Uma Pesquisa Bibliográfica PDFDocument4 paginiAmbiente Nas Organizações e Turbulência Ambiental - Uma Pesquisa Bibliográfica PDFcor com poesiaÎncă nu există evaluări
- Peça Teatral o Monge Eo ExecutivoDocument11 paginiPeça Teatral o Monge Eo Executivocor com poesiaÎncă nu există evaluări
- PNL MetáforasDocument105 paginiPNL Metáforascor com poesia100% (1)
- Cap 5 Liderança B.em PrincípiosDocument18 paginiCap 5 Liderança B.em Princípioscor com poesiaÎncă nu există evaluări
- Calendário Técnico de Vacinação - AdolescenteDocument2 paginiCalendário Técnico de Vacinação - AdolescenteLuana RibeiroÎncă nu există evaluări
- Vacinas Extra Pnv-Ajuda Na Tomada de DecisoesDocument2 paginiVacinas Extra Pnv-Ajuda Na Tomada de DecisoesJPMÎncă nu există evaluări
- Guia Prático de VacinasDocument60 paginiGuia Prático de Vacinasbeque233100% (2)
- Doenças ImunopreveníveisDocument18 paginiDoenças ImunopreveníveisAlexandreÎncă nu există evaluări
- Apostila Educativa 8 AnoDocument3 paginiApostila Educativa 8 AnoE. M. Joaquim da Silva PeçanhaÎncă nu există evaluări
- Slides VírusDocument10 paginiSlides VírusJoão Pedro AleixoÎncă nu există evaluări
- Virus e Viroses - 3º Ano - Bio - 01Document58 paginiVirus e Viroses - 3º Ano - Bio - 01Igor CajatyÎncă nu există evaluări
- Covid TestDocument3 paginiCovid TestBro ZicÎncă nu există evaluări
- Apoiolab: Coronavírus Detecção Por PCR (Covid 19)Document3 paginiApoiolab: Coronavírus Detecção Por PCR (Covid 19)Lorenzo RolimÎncă nu există evaluări
- Exercícios Virologia 1a UnidadDocument8 paginiExercícios Virologia 1a UnidadMarcos LimaÎncă nu există evaluări
- Certificado Digital COVID UEDocument1 paginăCertificado Digital COVID UEAlberto FontesÎncă nu există evaluări
- Fundacentro PR Riscos Biolgicos - 31042011Document25 paginiFundacentro PR Riscos Biolgicos - 31042011Leandro KovalickÎncă nu există evaluări
- Aula 01 - VirologiaDocument28 paginiAula 01 - Virologiagracelia fernandesÎncă nu există evaluări
- Especialidade de Vírus RespondidaDocument6 paginiEspecialidade de Vírus RespondidaArtur HenriqueÎncă nu există evaluări
- Resumo Perguntas DermatovirosesDocument8 paginiResumo Perguntas DermatovirosesYasminÎncă nu există evaluări
- Cobreiro - o Que É, Sintomas, Causas e Tratamento - Tua SaúdeDocument4 paginiCobreiro - o Que É, Sintomas, Causas e Tratamento - Tua SaúdeMauro VianaÎncă nu există evaluări
- A Infecção Do Vírus HIV No Hospedeiro Humano DefinitivoDocument38 paginiA Infecção Do Vírus HIV No Hospedeiro Humano Definitivoapi-3713502100% (1)
- Livro - Processo de Enfermagem - Wanda HortaDocument9 paginiLivro - Processo de Enfermagem - Wanda HortaJordana SouzaÎncă nu există evaluări
- NR 07 - Calendário de Vacinação OcupacionalDocument2 paginiNR 07 - Calendário de Vacinação OcupacionalCPSSTÎncă nu există evaluări
- Tics - Semana 06Document3 paginiTics - Semana 06enizia.silvaÎncă nu există evaluări
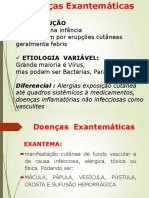
- Doenças Exantemáticas 2017 PDFDocument45 paginiDoenças Exantemáticas 2017 PDFMarcell CoutinhoÎncă nu există evaluări
- Antivirais 2016 - ComplementadoDocument65 paginiAntivirais 2016 - ComplementadoFagner LimaÎncă nu există evaluări
- 1333139016interpretacao de Testes Hepatite PDFDocument1 pagină1333139016interpretacao de Testes Hepatite PDFFabio Luis BusseÎncă nu există evaluări
- Cartão de VacinaDocument3 paginiCartão de VacinaVanessa NogueiraÎncă nu există evaluări
- Atestados 2022Document25 paginiAtestados 2022José Marcos Wanderley Marcos WanderleyÎncă nu există evaluări
- DGS VASPR e A Alergia Ao Ovo PDFDocument3 paginiDGS VASPR e A Alergia Ao Ovo PDFSara Afonso AzevedoÎncă nu există evaluări
- Calend Sbim 0 100 2022 2023Document1 paginăCalend Sbim 0 100 2022 2023UBS Francisco Marcos BatistaÎncă nu există evaluări
- Herpes Vírus HumanoDocument109 paginiHerpes Vírus HumanoSamuel MachadoÎncă nu există evaluări
- Plano de Ensino Virologia 2024 Maria Cristina Carlan Da SilvaDocument4 paginiPlano de Ensino Virologia 2024 Maria Cristina Carlan Da Silvapriscila.nascimentoÎncă nu există evaluări
- Herpes VírusDocument1 paginăHerpes VírusMafalda RealinhoÎncă nu există evaluări
- Fogo no parquinho: Namoro à luz da Palavra de DeusDe la EverandFogo no parquinho: Namoro à luz da Palavra de DeusEvaluare: 5 din 5 stele5/5 (9)
- Disciplina positiva para pais de crianças com autismoDe la EverandDisciplina positiva para pais de crianças com autismoÎncă nu există evaluări
- 21 dias para curar sua vida: Amando a si mesmo trabalhando com o espelhoDe la Everand21 dias para curar sua vida: Amando a si mesmo trabalhando com o espelhoEvaluare: 4.5 din 5 stele4.5/5 (49)
- Corpo como Palavra: Uma visão bíblica sobre saúde integralDe la EverandCorpo como Palavra: Uma visão bíblica sobre saúde integralEvaluare: 5 din 5 stele5/5 (1)
- Encantamentos, Rezas E BenzedurasDe la EverandEncantamentos, Rezas E BenzedurasEvaluare: 4.5 din 5 stele4.5/5 (11)
- Deu a louca nos signos: Um guia divertido do zodíaco por AstroloucamenteDe la EverandDeu a louca nos signos: Um guia divertido do zodíaco por AstroloucamenteEvaluare: 5 din 5 stele5/5 (1)
- Descolonizando afetos: Experimentações sobre outras formas de amarDe la EverandDescolonizando afetos: Experimentações sobre outras formas de amarEvaluare: 5 din 5 stele5/5 (6)
- Magias, Feitiços, Rituais E Simpatias De São Cipriano Em PdfDe la EverandMagias, Feitiços, Rituais E Simpatias De São Cipriano Em PdfEvaluare: 5 din 5 stele5/5 (3)
- Eu te amo, mas não te quero mais: Histórias de fins e recomeçosDe la EverandEu te amo, mas não te quero mais: Histórias de fins e recomeçosEvaluare: 5 din 5 stele5/5 (6)
- Desbloqueie o poder da sua mente: Programe o seu subconsciente para se libertar das dores e inseguranças e transforme a sua vidaDe la EverandDesbloqueie o poder da sua mente: Programe o seu subconsciente para se libertar das dores e inseguranças e transforme a sua vidaEvaluare: 4.5 din 5 stele4.5/5 (226)
- O fim da ansiedade: O segredo bíblico para livrar-se das preocupaçõesDe la EverandO fim da ansiedade: O segredo bíblico para livrar-se das preocupaçõesEvaluare: 5 din 5 stele5/5 (16)
- Nana Nenê: Como cuidar de seu bebê para que durma a noite toda de forma naturalDe la EverandNana Nenê: Como cuidar de seu bebê para que durma a noite toda de forma naturalEvaluare: 4.5 din 5 stele4.5/5 (5)
- Crianças desafiadoras: Aprenda como identificar, tratar e contribuir de maneira positiva com crianças que têm Transtorno Opositivo-DesafiadorDe la EverandCrianças desafiadoras: Aprenda como identificar, tratar e contribuir de maneira positiva com crianças que têm Transtorno Opositivo-DesafiadorÎncă nu există evaluări
- As 5 linguagens do amor - 3ª edição: Como expressar um compromisso de amor a seu cônjugeDe la EverandAs 5 linguagens do amor - 3ª edição: Como expressar um compromisso de amor a seu cônjugeEvaluare: 5 din 5 stele5/5 (220)
- Almanaque do Pensamento 2024: Guia astrológico para 2024De la EverandAlmanaque do Pensamento 2024: Guia astrológico para 2024Evaluare: 5 din 5 stele5/5 (2)
- Rumo aos 120 Anos: Como desfrutar a realidade bíblica e científica de uma vida longa e plenaDe la EverandRumo aos 120 Anos: Como desfrutar a realidade bíblica e científica de uma vida longa e plenaEvaluare: 5 din 5 stele5/5 (1)
- Expansão da Consciência: A Verdadeira História da Humanidade e a Transição PlanetáriaDe la EverandExpansão da Consciência: A Verdadeira História da Humanidade e a Transição PlanetáriaEvaluare: 5 din 5 stele5/5 (1)
- O Verdadeiro Ho'oponopono: Como restaurar sua harmonia, limpar memórias e manifestar milagresDe la EverandO Verdadeiro Ho'oponopono: Como restaurar sua harmonia, limpar memórias e manifestar milagresEvaluare: 5 din 5 stele5/5 (5)
- As 10 Leis Secretas da Visualização: Como Aplicar a Arte da Projeção Mental Para Obter SucessoDe la EverandAs 10 Leis Secretas da Visualização: Como Aplicar a Arte da Projeção Mental Para Obter SucessoEvaluare: 4.5 din 5 stele4.5/5 (5)
- Banhos, Defumações, Encantamentos, Feitiços, Magias, Oferendas, Rituais E Simpatias De Maria PadilhaDe la EverandBanhos, Defumações, Encantamentos, Feitiços, Magias, Oferendas, Rituais E Simpatias De Maria PadilhaEvaluare: 5 din 5 stele5/5 (1)
- Herbologia Mágica: A cura pela Natureza com base na Fitoterapia & Botânica OcultaDe la EverandHerbologia Mágica: A cura pela Natureza com base na Fitoterapia & Botânica OcultaEvaluare: 4.5 din 5 stele4.5/5 (7)