S-ar putea să vă placă și
- Urology DossierDocument166 paginiUrology DossierPeterÎncă nu există evaluări
- Lecture Notes Urology Pages 271 277Document7 paginiLecture Notes Urology Pages 271 277Beso Davitashvili0% (1)
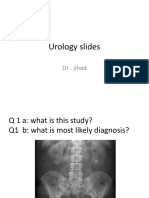
- Urology Slides: DR - JihadDocument4 paginiUrology Slides: DR - JihadJihad Anad100% (1)
- Urology 90 Seconds - Buku 1Document202 paginiUrology 90 Seconds - Buku 1Ari Alauddin100% (1)
- Urology Essay QuestionsDocument2 paginiUrology Essay QuestionsPeter AbikoyeÎncă nu există evaluări
- Urology NotesDocument33 paginiUrology NotesRight VentricleÎncă nu există evaluări
- Urology Complete Qbank PDFDocument58 paginiUrology Complete Qbank PDFPanda Panda100% (1)
- Uro RadiologyDocument78 paginiUro RadiologyDavid Ogechi Atandi100% (1)
- Physiologic Monitoring of The Surgical PatientDocument56 paginiPhysiologic Monitoring of The Surgical PatientSeid Adem100% (2)
- Head & Neck: Most CommonDocument6 paginiHead & Neck: Most CommonJüdith Marie Reyes BauntoÎncă nu există evaluări
- Sacrococcygeal Teratoma - Paediatric Surgery UnitDocument74 paginiSacrococcygeal Teratoma - Paediatric Surgery UnitOsasumwen OsagieÎncă nu există evaluări
- Surgery Viva QuestionsDocument16 paginiSurgery Viva QuestionsChris Lam Cui ShanÎncă nu există evaluări
- Exam Osce 3Document37 paginiExam Osce 3momo100% (1)
- Absite January2014 ReviewDocument1.226 paginiAbsite January2014 ReviewAnnTran100% (12)
- Chapter 34 Pediatric SurgeryDocument11 paginiChapter 34 Pediatric SurgeryMike G100% (1)
- 5 Surgery PreTest Self-Assessment and Review 13th Edition-Pages-47-57,39-43Document16 pagini5 Surgery PreTest Self-Assessment and Review 13th Edition-Pages-47-57,39-43Mae Rose Charlene MendozaÎncă nu există evaluări
- Cardiology OSCEDocument35 paginiCardiology OSCEvigneshmmc02Încă nu există evaluări
- Colorectal Oral Boards ReviewDocument79 paginiColorectal Oral Boards Revieweztouch12Încă nu există evaluări
- NMT11 Urology Special NoteDocument36 paginiNMT11 Urology Special NoteYiba Zul100% (4)
- Schwartz Chapter 33 SpleenDocument20 paginiSchwartz Chapter 33 SpleenGay Solas Epalan100% (1)
- UrologyDocument36 paginiUrologyakufahaba100% (2)
- Surgery-1 NotesDocument186 paginiSurgery-1 NotesSaadan Ahmed100% (1)
- (CLINICS) Surgery Notes +CPGDocument53 pagini(CLINICS) Surgery Notes +CPGEmily LaurenteÎncă nu există evaluări
- Eras For Psgs Review 2018Document18 paginiEras For Psgs Review 2018Gianina DelgadoÎncă nu există evaluări
- 5B Surgery 1st-2nd SE #28-32 #17-18Document3 pagini5B Surgery 1st-2nd SE #28-32 #17-18Liza SoberkaayoÎncă nu există evaluări
- C 10 + 11 GALLBLADDER AND BILIARY TRACT Part1Document45 paginiC 10 + 11 GALLBLADDER AND BILIARY TRACT Part1mikaaa0000% (1)
- Ashley Esdaile MSIII Byron Baptist MSIII Mike Pothen MS IIIDocument77 paginiAshley Esdaile MSIII Byron Baptist MSIII Mike Pothen MS IIISutapa PawarÎncă nu există evaluări
- Q Bank SurgeryDocument161 paginiQ Bank Surgerynawaf millionÎncă nu există evaluări
- Clinical UrologyDocument98 paginiClinical Urologythapan87100% (2)
- Pediatric Surgery 2 (Respiratory and Gastrointestinal Conditions) PDFDocument12 paginiPediatric Surgery 2 (Respiratory and Gastrointestinal Conditions) PDFRenatoCosmeGalvanJunior100% (1)
- Surgery McqsDocument10 paginiSurgery McqsSoodn Kang SoodnÎncă nu există evaluări
- 5 6057345046456304562Document490 pagini5 6057345046456304562DK DeepakÎncă nu există evaluări
- OPHTHA TransDocument10 paginiOPHTHA TransanonymousÎncă nu există evaluări
- Benign Gynecologic LesionsDocument103 paginiBenign Gynecologic Lesions201286% (7)
- Intern TicklerDocument10 paginiIntern TicklerRem AlfelorÎncă nu există evaluări
- Scrotal SwellingDocument63 paginiScrotal SwellingTommysÎncă nu există evaluări
- OSPE 4th Yr PathoDocument144 paginiOSPE 4th Yr PathoMuhammadShahzadÎncă nu există evaluări
- TOPIC NAME-GP Urology MCQsDocument9 paginiTOPIC NAME-GP Urology MCQsAsif Newaz100% (1)
- Mini Osce 1 PDFDocument138 paginiMini Osce 1 PDFabdelaheem arabiatÎncă nu există evaluări
- (Surg2) 5.4 Urology Part 3Document23 pagini(Surg2) 5.4 Urology Part 3AlloiBialbaÎncă nu există evaluări
- Medical Facts and Mcq's Urology MCQDocument14 paginiMedical Facts and Mcq's Urology MCQSmart Urosurgeon100% (2)
- Systemic Surgery NuggetsDocument17 paginiSystemic Surgery NuggetsAhmad UsmanÎncă nu există evaluări
- Urology NotesDocument8 paginiUrology NotesCzarinah Bacuado67% (3)
- Breast Absite QuestionsDocument18 paginiBreast Absite QuestionsGeshabelle ApuraÎncă nu există evaluări
- 1.40 (Surgery) GIT Surgical Diseases - Diagnostics - Obesity ManagementDocument10 pagini1.40 (Surgery) GIT Surgical Diseases - Diagnostics - Obesity ManagementLeo Mari Go LimÎncă nu există evaluări
- Surgery OsceDocument69 paginiSurgery OsceRebecca BrandonÎncă nu există evaluări
- 08.blueprints Surgery 5th EdDocument70 pagini08.blueprints Surgery 5th EdFadi AlkhassawnehÎncă nu există evaluări
- Schwartz UrologyDocument10 paginiSchwartz UrologyRem Alfelor100% (1)
- Surgery Mock 1Document7 paginiSurgery Mock 1aa.Încă nu există evaluări
- HX Taking of PeadiatricsDocument5 paginiHX Taking of PeadiatricsCahaya Al-Hazeenillah100% (1)
- Surgery Oral Exam TopicsDocument115 paginiSurgery Oral Exam Topicsmange24Încă nu există evaluări
- Urology Case Presentation - Scrotal Mass 1Document20 paginiUrology Case Presentation - Scrotal Mass 1Hakimah K. Suhaimi100% (1)
- Urology Quiz PDFDocument7 paginiUrology Quiz PDFParsaant Singh100% (1)
- Investigations in UrologyDocument19 paginiInvestigations in UrologyMohammed AadeelÎncă nu există evaluări
- CC Silva - Rationalization 2022Document35 paginiCC Silva - Rationalization 2022Nicole Xyza JunsayÎncă nu există evaluări
- University of Perpetual Help Rizal Jonelta Foundation School of Medicine Department of Surgery - ConsortiumDocument17 paginiUniversity of Perpetual Help Rizal Jonelta Foundation School of Medicine Department of Surgery - Consortiummefav7778520Încă nu există evaluări
- 4.kidneys, Ureters and Suprarenal GlandsDocument57 pagini4.kidneys, Ureters and Suprarenal GlandsIshimwe TheotimeÎncă nu există evaluări
- AUBF Lec Renal Function I PDFDocument4 paginiAUBF Lec Renal Function I PDFBanana QÎncă nu există evaluări
- Yusi - Anatomy of The Urinary Tract 2009 12-7Document129 paginiYusi - Anatomy of The Urinary Tract 2009 12-7abstabsÎncă nu există evaluări
- L31 - Renal SystemDocument30 paginiL31 - Renal SystemsairahhannahÎncă nu există evaluări
- Cannabis As Cause of Death Drummer2019Document9 paginiCannabis As Cause of Death Drummer2019yossiÎncă nu există evaluări
- Mark Scheme (Provisional) Summer 2021: Pearson Edexcel International GCSE in Biology (4BI1) Paper 2BDocument17 paginiMark Scheme (Provisional) Summer 2021: Pearson Edexcel International GCSE in Biology (4BI1) Paper 2BThakoon TtsÎncă nu există evaluări
- Mark Scheme (Results) January 2021: Pearson Edexcel International GCSE in Biology (4BI1) Paper 2BRDocument16 paginiMark Scheme (Results) January 2021: Pearson Edexcel International GCSE in Biology (4BI1) Paper 2BRThakoon TtsÎncă nu există evaluări
- January 2021 P2BR QPDocument24 paginiJanuary 2021 P2BR QPSareeha SadhviÎncă nu există evaluări
- Mark Scheme (Provisional) Summer 2021: Pearson Edexcel International GCSE in Biology (4BI1) Paper 2BDocument17 paginiMark Scheme (Provisional) Summer 2021: Pearson Edexcel International GCSE in Biology (4BI1) Paper 2BThakoon TtsÎncă nu există evaluări
- Unger Et Al 2020 2020 International Society of Hypertension Global Hypertension Practice GuidelinesDocument24 paginiUnger Et Al 2020 2020 International Society of Hypertension Global Hypertension Practice GuidelinesEduardo Marco Villarama DayritÎncă nu există evaluări
- January 2021 P2BR QPDocument24 paginiJanuary 2021 P2BR QPSareeha SadhviÎncă nu există evaluări
- Monday 1 June 2020: BiologyDocument20 paginiMonday 1 June 2020: BiologyAdeeba iqbal100% (2)
- Eng ชุดที่3 4Document26 paginiEng ชุดที่3 4Thakoon TtsÎncă nu există evaluări
- Mark Scheme (Results) November 2020: Pearson Edexcel International GCSE in Biology (4BI1) Paper 2BDocument19 paginiMark Scheme (Results) November 2020: Pearson Edexcel International GCSE in Biology (4BI1) Paper 2BThakoon TtsÎncă nu există evaluări
- Mark Scheme (Results) January 2021: Pearson Edexcel International GCSE in Biology (4BI1) Paper 2BDocument25 paginiMark Scheme (Results) January 2021: Pearson Edexcel International GCSE in Biology (4BI1) Paper 2BThakoon TtsÎncă nu există evaluări
- Monday 1 June 2020: BiologyDocument20 paginiMonday 1 June 2020: BiologyAdeeba iqbal100% (2)
- Monday 1 June 2020: BiologyDocument16 paginiMonday 1 June 2020: BiologyThakoon TtsÎncă nu există evaluări
- Placental AbnormalitiesDocument3 paginiPlacental AbnormalitiesThakoon TtsÎncă nu există evaluări
- 13.topical Steroid Usage-2011 PDFDocument8 pagini13.topical Steroid Usage-2011 PDFThakoon TtsÎncă nu există evaluări
- Mark Scheme (Results) November 2020: Pearson Edexcel International GCSE in Biology (4BI1) Paper 2BRDocument16 paginiMark Scheme (Results) November 2020: Pearson Edexcel International GCSE in Biology (4BI1) Paper 2BRThakoon TtsÎncă nu există evaluări
- Subspec Urology: GU TumorsDocument5 paginiSubspec Urology: GU TumorsThakoon TtsÎncă nu există evaluări
- Skin & Subcutaneous TissueDocument10 paginiSkin & Subcutaneous TissueThakoon TtsÎncă nu există evaluări
- PEDIA Neuromuscular DisorderDocument3 paginiPEDIA Neuromuscular DisorderThakoon TtsÎncă nu există evaluări
- Prostate Gland: Delay in StartingDocument2 paginiProstate Gland: Delay in StartingThakoon TtsÎncă nu există evaluări
- Urinary StoneDocument5 paginiUrinary StoneThakoon TtsÎncă nu există evaluări
- ENT - Diseases of The Inner Ear 2014Document4 paginiENT - Diseases of The Inner Ear 2014Thakoon TtsÎncă nu există evaluări
- P2 Breast Pathology (Patho Surg) PDFDocument120 paginiP2 Breast Pathology (Patho Surg) PDFThakoon TtsÎncă nu există evaluări
- ENT - Dse of Inner EarDocument7 paginiENT - Dse of Inner EarThakoon TtsÎncă nu există evaluări
- Antiprotozoal Agents: Pharmacology Group III Beguas, Beltran, Bejawada, Bingari, Cabrera, Cadawas, CaliwagDocument86 paginiAntiprotozoal Agents: Pharmacology Group III Beguas, Beltran, Bejawada, Bingari, Cabrera, Cadawas, CaliwagThakoon TtsÎncă nu există evaluări
- Common GI Signs and SymptomsDocument66 paginiCommon GI Signs and SymptomsThakoon TtsÎncă nu există evaluări
- Diseases of The Immune SystemDocument19 paginiDiseases of The Immune SystemThakoon TtsÎncă nu există evaluări
- EAR Anatomy, Physiology, Embryology & Congenital AnomalyDocument6 paginiEAR Anatomy, Physiology, Embryology & Congenital AnomalyThakoon TtsÎncă nu există evaluări
- Common Gi Signs and SymptomsDocument11 paginiCommon Gi Signs and SymptomsThakoon TtsÎncă nu există evaluări
- Case 4Document6 paginiCase 4Azmi AzzahraÎncă nu există evaluări
- SJFJFDocument9 paginiSJFJFcharizze alpechiÎncă nu există evaluări
- Bladder Outlet Obstruction in Children PDFDocument64 paginiBladder Outlet Obstruction in Children PDFalaaÎncă nu există evaluări
- Nursing Care Plan For Benign Prostatic Hypertrophy NCPDocument9 paginiNursing Care Plan For Benign Prostatic Hypertrophy NCPderic88% (8)
- Urethral Pathology: Case 1 Case 2Document2 paginiUrethral Pathology: Case 1 Case 2HardiTariqHammaÎncă nu există evaluări
- Benign Prostatic Hyperplasia Is A BenignDocument4 paginiBenign Prostatic Hyperplasia Is A BenignZeinab SrourÎncă nu există evaluări
- Guidelines On Pain ManagementDocument85 paginiGuidelines On Pain ManagementmelawatiÎncă nu există evaluări
- UNIT 10 (Urinary System)Document6 paginiUNIT 10 (Urinary System)Workinesh Kaynabo KambaloÎncă nu există evaluări
- Urinary SystemDocument64 paginiUrinary Systemazlidai ismailÎncă nu există evaluări
- Obstructive UropathyDocument8 paginiObstructive UropathyTeslim Raji100% (1)
- An Assi Gnment On Cat Het Eri Zat I OnDocument17 paginiAn Assi Gnment On Cat Het Eri Zat I OnGyanbhushan BhartiÎncă nu există evaluări
- Anatomy and Physiology of Urinary SystemDocument61 paginiAnatomy and Physiology of Urinary SystemBhusan TamrakarÎncă nu există evaluări
- Zoology Finals ReviewerDocument18 paginiZoology Finals ReviewerZian Lei MienÎncă nu există evaluări
- Surgical Female Urogenital Anatomy - UpToDateDocument57 paginiSurgical Female Urogenital Anatomy - UpToDateErickÎncă nu există evaluări
- Radiology SPOTTERS 1Document34 paginiRadiology SPOTTERS 1Sivakumar SadasivamÎncă nu există evaluări
- Declaration of Good Health Form - With Covid QDocument2 paginiDeclaration of Good Health Form - With Covid QRajnish YadavÎncă nu există evaluări
- Gross Anatomy of Uterus: D R. Vibhash Kumar Vaidya Department of AnatomyDocument25 paginiGross Anatomy of Uterus: D R. Vibhash Kumar Vaidya Department of AnatomyAhsan TariqÎncă nu există evaluări
- Case Study-Acute Urinary RetentionDocument10 paginiCase Study-Acute Urinary RetentionArthadian De Peralta75% (4)
- MRCOG Part 1 HijauDocument367 paginiMRCOG Part 1 HijaurifkiÎncă nu există evaluări
- Uti in PregnancyDocument27 paginiUti in PregnancyShiney Rhet DACULAÎncă nu există evaluări
- Ncbi - Nlm.nih - Gov-Post-Op Urinary RetentionDocument9 paginiNcbi - Nlm.nih - Gov-Post-Op Urinary RetentiondadupipaÎncă nu există evaluări
- A Nursing Case StudyDocument105 paginiA Nursing Case StudyStephen Tumbaga75% (4)
- UTI Prevention Fact SheetDocument1 paginăUTI Prevention Fact Sheetalifia alqibtiaÎncă nu există evaluări
- Neural Control of BladderDocument37 paginiNeural Control of BladderPalak EnginirÎncă nu există evaluări
- Science6 Qtr2 Set1-FinalDocument32 paginiScience6 Qtr2 Set1-FinalLady Jae ArbesoÎncă nu există evaluări
- Human Reflex Physiology: ExerciseDocument4 paginiHuman Reflex Physiology: ExerciseGlainee esor selfroÎncă nu există evaluări
- Medical Surgical Nursing: Gracious Colleg of Nursing Abhanpur Raipur (C.G.)Document9 paginiMedical Surgical Nursing: Gracious Colleg of Nursing Abhanpur Raipur (C.G.)Topeshwar TpkÎncă nu există evaluări
- Cystoscopy - Mayo ClinicDocument7 paginiCystoscopy - Mayo ClinicSAIFUL ISLAMÎncă nu există evaluări
- External and Internal Anatomy of FISHDocument22 paginiExternal and Internal Anatomy of FISHsheil.cogayÎncă nu există evaluări
- MCN ExamDocument13 paginiMCN ExamtinaÎncă nu există evaluări
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDe la EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsÎncă nu există evaluări
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDe la EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisEvaluare: 4.5 din 5 stele4.5/5 (42)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeEvaluare: 2 din 5 stele2/5 (1)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDe la EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsEvaluare: 5 din 5 stele5/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe la EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityEvaluare: 4 din 5 stele4/5 (24)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDe la EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedEvaluare: 5 din 5 stele5/5 (80)
- The Obesity Code: Unlocking the Secrets of Weight LossDe la EverandThe Obesity Code: Unlocking the Secrets of Weight LossEvaluare: 4 din 5 stele4/5 (6)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDe la EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDe la EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsEvaluare: 4.5 din 5 stele4.5/5 (169)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDe la EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDEvaluare: 5 din 5 stele5/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDe la EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityEvaluare: 4 din 5 stele4/5 (3)
- Gut: the new and revised Sunday Times bestsellerDe la EverandGut: the new and revised Sunday Times bestsellerEvaluare: 4 din 5 stele4/5 (392)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDe la EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeEvaluare: 4.5 din 5 stele4.5/5 (253)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDe la EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsEvaluare: 3.5 din 5 stele3.5/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisDe la EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisEvaluare: 3.5 din 5 stele3.5/5 (2)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningDe la EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningEvaluare: 4 din 5 stele4/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.De la EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Evaluare: 4.5 din 5 stele4.5/5 (110)
- To Explain the World: The Discovery of Modern ScienceDe la EverandTo Explain the World: The Discovery of Modern ScienceEvaluare: 3.5 din 5 stele3.5/5 (51)
- An Autobiography of Trauma: A Healing JourneyDe la EverandAn Autobiography of Trauma: A Healing JourneyEvaluare: 5 din 5 stele5/5 (2)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDe la EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessEvaluare: 4.5 din 5 stele4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDe la EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisEvaluare: 4 din 5 stele4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDe la EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryEvaluare: 4 din 5 stele4/5 (44)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisDe la EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisEvaluare: 4 din 5 stele4/5 (9)