S-ar putea să vă placă și
- CNS NeurotransmittersDocument30 paginiCNS Neurotransmittersdevanshi_582262183100% (1)
- Unit 1: Psychotherapy: But The Current Definition of Psychotherapy Is Board - I.EDocument59 paginiUnit 1: Psychotherapy: But The Current Definition of Psychotherapy Is Board - I.EabrihamÎncă nu există evaluări
- Neurotransmitters-Classification, Relevance in The Etiology and Treatment of Mental IllnessDocument22 paginiNeurotransmitters-Classification, Relevance in The Etiology and Treatment of Mental Illnessneethus10Încă nu există evaluări
- Mockery Breed Murder Birds PDFDocument12 paginiMockery Breed Murder Birds PDFLautaro BojanichÎncă nu există evaluări
- CheckList For Checking of Drawings-R1Document4 paginiCheckList For Checking of Drawings-R1jatin kalraÎncă nu există evaluări
- Flow Chart - QCDocument2 paginiFlow Chart - QCKarthikeyan Shanmugavel100% (1)
- NeurotransmittersDocument92 paginiNeurotransmittersClare DucutÎncă nu există evaluări
- Neurotransmitters and Intro To NeuropeptidesDocument566 paginiNeurotransmitters and Intro To NeuropeptidesJAH100% (3)
- Geriatric Psychiatry LectureDocument113 paginiGeriatric Psychiatry LectureabrihamÎncă nu există evaluări
- E.2 Bipolar PPT 2017Document42 paginiE.2 Bipolar PPT 2017abrihamÎncă nu există evaluări
- Chapter 3 Brain and BehaviourDocument46 paginiChapter 3 Brain and Behaviour038 Suri HananÎncă nu există evaluări
- NeurotransmittersDocument29 paginiNeurotransmittersashupathakaÎncă nu există evaluări
- Neurotransmitter Release and ProcessDocument14 paginiNeurotransmitter Release and ProcessRain TolentinoÎncă nu există evaluări
- ACETYLCHOLINEDocument50 paginiACETYLCHOLINEAps100% (1)
- NeuropeptidesDocument62 paginiNeuropeptidesshankarkjs1983Încă nu există evaluări
- Neurotransmission Notes 3Document4 paginiNeurotransmission Notes 3api-188978784Încă nu există evaluări
- Neuro TransmitatorDocument70 paginiNeuro TransmitatorVlad Si Camelia RachieruÎncă nu există evaluări
- Introduction To NeurotransmittersDocument27 paginiIntroduction To NeurotransmittersSuri khairatiÎncă nu există evaluări
- Neurotransmitters 1Document23 paginiNeurotransmitters 1Preety ShresthaÎncă nu există evaluări
- Provision of EPCI Services For EPCIC Sidayu Wellhead Platforms and Pipelines Sidayu Field DevelopmentDocument7 paginiProvision of EPCI Services For EPCIC Sidayu Wellhead Platforms and Pipelines Sidayu Field Developmentriandi100% (1)
- Brain and Behavior: Hyacinth C. Manood, MD, FppaDocument16 paginiBrain and Behavior: Hyacinth C. Manood, MD, FppaSangamesh Sarja100% (1)
- Sustainable Events Guide May 30 2012 FINAL PDFDocument118 paginiSustainable Events Guide May 30 2012 FINAL PDFInter 4DMÎncă nu există evaluări
- Naming Hydrocarbons Worksheet1 Key 12 26 08 PDFDocument2 paginiNaming Hydrocarbons Worksheet1 Key 12 26 08 PDFMarilyn Castro Laquindanum100% (1)
- Sleep Disorders: Daniel F. Kripke, MDDocument122 paginiSleep Disorders: Daniel F. Kripke, MDabrihamÎncă nu există evaluări
- Farmakologija Cns-A Sa Osvrtom Na Hemijske Medijatore - Seminarski RadDocument63 paginiFarmakologija Cns-A Sa Osvrtom Na Hemijske Medijatore - Seminarski RadMelinda Dervic100% (1)
- Neurotransmitters And Anterior Pituitary FunctionDe la EverandNeurotransmitters And Anterior Pituitary FunctionÎncă nu există evaluări
- 5G Transport Slice Control in End-To-End 5G NetworksDocument19 pagini5G Transport Slice Control in End-To-End 5G NetworksmorganÎncă nu există evaluări
- Neurotransmitter: Harliansyah, PH.D Fakultas Kedokteran 2015Document25 paginiNeurotransmitter: Harliansyah, PH.D Fakultas Kedokteran 2015Cah NgitriÎncă nu există evaluări
- 3 - NeurotransmittersDocument23 pagini3 - NeurotransmittersupbandaraÎncă nu există evaluări
- Pharmacological Organization of The CNSDocument8 paginiPharmacological Organization of The CNSLeo PerezÎncă nu există evaluări
- Neurotransmitter: Harliansyah, PH.D Fakultas Kedokteran Dec'2016Document35 paginiNeurotransmitter: Harliansyah, PH.D Fakultas Kedokteran Dec'2016UlfaTitiswariÎncă nu există evaluări
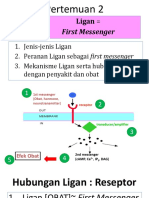
- 2-Ligan-First MassengerDocument33 pagini2-Ligan-First MassengerWahid AdvÎncă nu există evaluări
- 2 Ligan First MassengerDocument32 pagini2 Ligan First MassengerikhararaÎncă nu există evaluări
- Neurotransmitter (Dr. Devi) - 2Document71 paginiNeurotransmitter (Dr. Devi) - 2nazyaÎncă nu există evaluări
- Neurotransmitters - 2016Document183 paginiNeurotransmitters - 2016AdminÎncă nu există evaluări
- Pharm1 Blockii 17Document90 paginiPharm1 Blockii 17aksonarain1 23Încă nu există evaluări
- Phyp W4Document3 paginiPhyp W4SJÎncă nu există evaluări
- Presentation NeuronDocument7 paginiPresentation Neuronsuweino_harunÎncă nu există evaluări
- Part I. Principles of PsychopharmacologyDocument12 paginiPart I. Principles of PsychopharmacologyGauri SharmaÎncă nu există evaluări
- Neurotransmitter AgainDocument17 paginiNeurotransmitter Againsuweino_harunÎncă nu există evaluări
- Neurotransmitters and PsychopathologyDocument6 paginiNeurotransmitters and PsychopathologytakenotesanyaÎncă nu există evaluări
- Antidepressant and AntimanicDocument60 paginiAntidepressant and Antimanictbuyinza21apÎncă nu există evaluări
- Neurotransmitter 2Document37 paginiNeurotransmitter 2Preety ShresthaÎncă nu există evaluări
- Reviewer of A PsychologyDocument55 paginiReviewer of A PsychologyCAMMILLE EDZ FERRAS SELONGÎncă nu există evaluări
- NCM 106 Finals For PrintingDocument13 paginiNCM 106 Finals For PrintingJULIANNAH ATHENA MERCADOÎncă nu există evaluări
- Business: Reminder: Study For Quiz #2Document43 paginiBusiness: Reminder: Study For Quiz #2Melanie GaledoÎncă nu există evaluări
- Endocrine System: Chemical ControlDocument36 paginiEndocrine System: Chemical ControlGary VlaicuÎncă nu există evaluări
- Introduction of Pharmacology of Cns 29022024 031838pmDocument51 paginiIntroduction of Pharmacology of Cns 29022024 031838pmaz.rah.e.khudiÎncă nu există evaluări
- Kuliah VIII - Sistem Endokrin - KKPMT IIDocument50 paginiKuliah VIII - Sistem Endokrin - KKPMT IIRae SenaÎncă nu există evaluări
- Introduction To Autonomic PharmacologyDocument44 paginiIntroduction To Autonomic PharmacologyZemburukaÎncă nu există evaluări
- Biokimia Syaraf Dan Otak: Biochemistry Department Hasanuddin UniversityDocument52 paginiBiokimia Syaraf Dan Otak: Biochemistry Department Hasanuddin Universityraynhard b. fandresÎncă nu există evaluări
- 04 NeurotransmisoresDocument34 pagini04 NeurotransmisoresSamuel Salar PadillaÎncă nu există evaluări
- ةيودلاا ملع - Pharmacology-2Document244 paginiةيودلاا ملع - Pharmacology-2tarekÎncă nu există evaluări
- Bayosayk 1P31P5 PDFDocument13 paginiBayosayk 1P31P5 PDFWystanÎncă nu există evaluări
- Pharmacology 011 - ANS 3Document9 paginiPharmacology 011 - ANS 3Kaye NeeÎncă nu există evaluări
- CH 4 NotesDocument20 paginiCH 4 NotesIt'sCurryAndRice PlusWaterÎncă nu există evaluări
- "Drugs and The Brain" Week 1 Minilecture 1 Organization and Overview of Weeks 1 - 3 (The Basic Science)Document24 pagini"Drugs and The Brain" Week 1 Minilecture 1 Organization and Overview of Weeks 1 - 3 (The Basic Science)Jud VerdaguerÎncă nu există evaluări
- Bylund 2014Document3 paginiBylund 2014Javier RiveraÎncă nu există evaluări
- Pathophysiological Role Ofneuropeptide-NeurotransmitterinteractionsDocument6 paginiPathophysiological Role Ofneuropeptide-Neurotransmitterinteractionscc vereÎncă nu există evaluări
- 7779087Document65 pagini7779087MohamedÎncă nu există evaluări
- 126-Article Text-513-1-10-20170524Document10 pagini126-Article Text-513-1-10-20170524Yosia KevinÎncă nu există evaluări
- Cholinergic and Adrenergic PharmacologyDocument40 paginiCholinergic and Adrenergic PharmacologyAhmad Adam AhmadÎncă nu există evaluări
- Endocrine Respiratory Reproductive Excretory Urinary Nervous Immune SysytemDocument185 paginiEndocrine Respiratory Reproductive Excretory Urinary Nervous Immune SysytemEms TeopeÎncă nu există evaluări
- 09 18 2006 Bio Medical Synapse GraduateDocument24 pagini09 18 2006 Bio Medical Synapse Graduateapi-3696530Încă nu există evaluări
- Biological Bases of Behavior: Neuro Hormones. GABA, Glycine Peptides (Opiates)Document35 paginiBiological Bases of Behavior: Neuro Hormones. GABA, Glycine Peptides (Opiates)Adeel AizadÎncă nu există evaluări
- NeurotransmittersDocument21 paginiNeurotransmittersYannie GomezÎncă nu există evaluări
- NP1 PDFDocument32 paginiNP1 PDFRajat AgrawalÎncă nu există evaluări
- 06b Pharmacology Learning Material Drugs Affecting The Autonomic Nervous SystemDocument23 pagini06b Pharmacology Learning Material Drugs Affecting The Autonomic Nervous SystemJewel Ramos GalinatoÎncă nu există evaluări
- Intro NeurologyDocument64 paginiIntro NeurologySaritha SvÎncă nu există evaluări
- Session 02 Psychobiological ConceptsDocument58 paginiSession 02 Psychobiological ConceptsMalakatete Mwaipojele-fÎncă nu există evaluări
- Session I. NeuropharmacologyDocument53 paginiSession I. NeuropharmacologyEsteban ValenzuelaÎncă nu există evaluări
- GIT ModifiedDocument94 paginiGIT ModifiedabrihamÎncă nu există evaluări
- Institute Date Preffered Exam Center (AA or Mekelle)Document12 paginiInstitute Date Preffered Exam Center (AA or Mekelle)abrihamÎncă nu există evaluări
- Internal Facility Report and Resupply Form (IFRR) OPD PHARMACY DUDocument11 paginiInternal Facility Report and Resupply Form (IFRR) OPD PHARMACY DUabrihamÎncă nu există evaluări
- Blank Ifrr Edited by AwokeDocument5 paginiBlank Ifrr Edited by AwokeabrihamÎncă nu există evaluări
- ANS DipDocument60 paginiANS DipabrihamÎncă nu există evaluări
- Histroy Taking and Physical ExaminationDocument23 paginiHistroy Taking and Physical ExaminationabrihamÎncă nu există evaluări
- Implanon A Projestin Only Hormonal Contraceptive ImplantDocument28 paginiImplanon A Projestin Only Hormonal Contraceptive ImplantabrihamÎncă nu există evaluări
- Psychiatric Disorders Specific To WomenDocument25 paginiPsychiatric Disorders Specific To WomenabrihamÎncă nu există evaluări
- 5 Child and Adolescence Psychiatry-1Document332 pagini5 Child and Adolescence Psychiatry-1abrihamÎncă nu există evaluări
- Anxiolytics & Hypnotics Drugs: Chapter FiveDocument21 paginiAnxiolytics & Hypnotics Drugs: Chapter FiveabrihamÎncă nu există evaluări
- Adigrat UniversityDocument16 paginiAdigrat UniversityabrihamÎncă nu există evaluări
- Psychiatric Disorders in Childhood and AdolescenceDocument81 paginiPsychiatric Disorders in Childhood and Adolescenceabriham100% (1)
- Beating The Blues: Depression in Older PatientsDocument39 paginiBeating The Blues: Depression in Older PatientsabrihamÎncă nu există evaluări
- Common Child Psychiatric DisordersDocument30 paginiCommon Child Psychiatric DisordersabrihamÎncă nu există evaluări
- Personality Disorders: Mudr. Martin Perna Dept. of Psychiatry, Masaryk University, BrnoDocument31 paginiPersonality Disorders: Mudr. Martin Perna Dept. of Psychiatry, Masaryk University, BrnoabrihamÎncă nu există evaluări
- Principles of Chemical NeurotransmissionDocument5 paginiPrinciples of Chemical NeurotransmissionabrihamÎncă nu există evaluări
- Adigrat UniversityDocument29 paginiAdigrat UniversityabrihamÎncă nu există evaluări
- Sony Cdm82a 82b Cmt-hpx11d Hcd-hpx11d Mechanical OperationDocument12 paginiSony Cdm82a 82b Cmt-hpx11d Hcd-hpx11d Mechanical OperationDanÎncă nu există evaluări
- 外贸专业术语Document13 pagini外贸专业术语邱建华Încă nu există evaluări
- TreesDocument69 paginiTreesADITYA GEHLAWATÎncă nu există evaluări
- JKJKJDocument3 paginiJKJKJjosecarlosvjÎncă nu există evaluări
- Process Costing Exercises Series 1Document23 paginiProcess Costing Exercises Series 1sarahbeeÎncă nu există evaluări
- Presentation On 4G TechnologyDocument23 paginiPresentation On 4G TechnologyFresh EpicÎncă nu există evaluări
- Dual Shield 7100 Ultra: Typical Tensile PropertiesDocument3 paginiDual Shield 7100 Ultra: Typical Tensile PropertiesDino Paul Castro HidalgoÎncă nu există evaluări
- tGr12OM CheResoBookU78910Document110 paginitGr12OM CheResoBookU78910Jamunanantha PranavanÎncă nu există evaluări
- American BreakfastDocument4 paginiAmerican BreakfastHamilton Valenzuela ChipongianÎncă nu există evaluări
- Impact of Retrofitting Existing Combined Heat and Power Plant With Polygeneration of Biomethane PDFDocument16 paginiImpact of Retrofitting Existing Combined Heat and Power Plant With Polygeneration of Biomethane PDFAwais Salman0% (1)
- 41z S4hana2021 Set-Up en XXDocument46 pagini41z S4hana2021 Set-Up en XXHussain MulthazimÎncă nu există evaluări
- Eng DS Epp-2314 1410Document2 paginiEng DS Epp-2314 1410MarkusAldoMaquÎncă nu există evaluări
- Ali Erdemir: Professional ExperienceDocument3 paginiAli Erdemir: Professional ExperienceDunkMeÎncă nu există evaluări
- Ficha Tecnica-Skyjack SJ3219 8mtDocument2 paginiFicha Tecnica-Skyjack SJ3219 8mtLESLY MILENA MORENO CORALÎncă nu există evaluări
- LG250CDocument2 paginiLG250CCarlosÎncă nu există evaluări
- LET General Math ReviewerDocument7 paginiLET General Math ReviewerMarco Rhonel Eusebio100% (1)
- 123 09-Printable Menu VORDocument2 pagini123 09-Printable Menu VORArmstrong TowerÎncă nu există evaluări
- Determination of Drop-Impact Resistance of Plastic BottlesDocument11 paginiDetermination of Drop-Impact Resistance of Plastic BottlesAndres BrañaÎncă nu există evaluări
- The Passion For Cacti and Other Succulents: June 2017Document140 paginiThe Passion For Cacti and Other Succulents: June 2017golf2010Încă nu există evaluări
- SSDsDocument3 paginiSSDsDiki Tri IndartaÎncă nu există evaluări
- Structural Analysis and Design of Pressure Hulls - The State of The Art and Future TrendsDocument118 paginiStructural Analysis and Design of Pressure Hulls - The State of The Art and Future TrendsRISHABH JAMBHULKARÎncă nu există evaluări
- Hopeless PlacesDocument1.304 paginiHopeless Placesmoreblessingmarvellous659Încă nu există evaluări
- Lecture 12Document8 paginiLecture 12Mechanical ZombieÎncă nu există evaluări