S-ar putea să vă placă și
- The Love DareDocument4 paginiThe Love DareJeffrey Portalanza100% (3)
- Natures Pharmacy E-BookDocument505 paginiNatures Pharmacy E-Bookcas100% (3)
- Sample SoapDocument9 paginiSample SoapDouglas Greg Cook90% (20)
- SOAP NoteDocument8 paginiSOAP NoteAnonymous p0y5mmLQÎncă nu există evaluări
- Gastrointestinal System: Chapter EighteenDocument32 paginiGastrointestinal System: Chapter Eighteenhayascent hilarioÎncă nu există evaluări
- Test Questions Internal MedicineDocument13 paginiTest Questions Internal MedicineJo Anne86% (7)
- Case Presentations in Arterial DiseaseDe la EverandCase Presentations in Arterial DiseaseEvaluare: 5 din 5 stele5/5 (1)
- CASE 3 MEDICINE JULY 10 2019 AcutePyeloDocument15 paginiCASE 3 MEDICINE JULY 10 2019 AcutePyeloTrisÎncă nu există evaluări
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicDe la EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicEvaluare: 5 din 5 stele5/5 (1)
- Pharmacology Charts PDFDocument88 paginiPharmacology Charts PDFMohamad Samir90% (10)
- Final Assessment Soap NoteDocument13 paginiFinal Assessment Soap Noteapi-494643478100% (3)
- Case Report VI Internal MedicineDocument13 paginiCase Report VI Internal MedicineGidu SaidÎncă nu există evaluări
- Constitutional: General Appearance: Healthy-Appearing, Well-Nourished, and Well-Developed. Level ofDocument10 paginiConstitutional: General Appearance: Healthy-Appearing, Well-Nourished, and Well-Developed. Level ofRichard ObinwankwoÎncă nu există evaluări
- Helicobacter Pylori InfectionDocument8 paginiHelicobacter Pylori InfectionNovitaÎncă nu există evaluări
- PEDIA Case 4.1. Dengue FeverDocument10 paginiPEDIA Case 4.1. Dengue Feverotartil_nimanÎncă nu există evaluări
- Soap 2Document5 paginiSoap 2api-456313554Încă nu există evaluări
- Pedia 1Document8 paginiPedia 1Jani MisterioÎncă nu există evaluări
- Health Assessment Project: Name: Ena Lewis Tutor: Sis Francis Group: 15Document27 paginiHealth Assessment Project: Name: Ena Lewis Tutor: Sis Francis Group: 15Blake KamminÎncă nu există evaluări
- Low Back PainDocument9 paginiLow Back PainDoc AchondoÎncă nu există evaluări
- Soap FamedDocument79 paginiSoap FamedJane GarciaÎncă nu există evaluări
- Property Relations Between Husband and WifeDocument37 paginiProperty Relations Between Husband and WifeIzzyMaxinoÎncă nu există evaluări
- Chief ComplaintDocument7 paginiChief ComplaintyohannesÎncă nu există evaluări
- Script For Notarial CommissionDocument2 paginiScript For Notarial Commissionfafa_mhedz90% (10)
- The Nursing Assessment of Peptic UlcerDocument14 paginiThe Nursing Assessment of Peptic UlcerVelia suwandiÎncă nu există evaluări
- Drug StudyDocument23 paginiDrug StudyReiche GomezÎncă nu există evaluări
- Case Clerking ApendicDocument15 paginiCase Clerking ApendicChen Cheng0% (1)
- Bagtas Vs HonSantos PDFDocument3 paginiBagtas Vs HonSantos PDFIzzyMaxinoÎncă nu există evaluări
- Cwu SurgeryDocument16 paginiCwu SurgeryAslah NabilahÎncă nu există evaluări
- Ramos V BaldoDocument3 paginiRamos V BaldoIzzyMaxinoÎncă nu există evaluări
- Case Clerking ApendicDocument15 paginiCase Clerking ApendicMelvin Khung100% (1)
- AbortionDocument16 paginiAbortionKim Lompot100% (1)
- Diabetes Mellitus Complte LONG 2Document56 paginiDiabetes Mellitus Complte LONG 2John Vincent Dy OcampoÎncă nu există evaluări
- Peptic Ulcer Disease (Pud) Concept Map PUDDocument1 paginăPeptic Ulcer Disease (Pud) Concept Map PUDIris Mambuay0% (1)
- Ward Paper LegitDocument13 paginiWard Paper LegitLuigi FranciscoÎncă nu există evaluări
- History 1Document11 paginiHistory 1KaleabÎncă nu există evaluări
- Acute PancreatitisDocument7 paginiAcute PancreatitisPatrick DycocoÎncă nu există evaluări
- Clinical Case: Section A - Group 8Document68 paginiClinical Case: Section A - Group 8madison Deli100% (1)
- 6904 Module 1 HistoryDocument3 pagini6904 Module 1 Historyapi-618492022Încă nu există evaluări
- Date and Time: June 23, 2018, 3PM Chief Complaint: Difficulty of Breathing History of Present IllnessDocument3 paginiDate and Time: June 23, 2018, 3PM Chief Complaint: Difficulty of Breathing History of Present IllnessConcepcion R. AquinoÎncă nu există evaluări
- 312 ENT Patient InterviewDocument5 pagini312 ENT Patient InterviewDorish Faith CarilloÎncă nu există evaluări
- Template Gyn Lo Abd PainDocument18 paginiTemplate Gyn Lo Abd PainHassan HarirÎncă nu există evaluări
- HISTORY # 1 - PCGH, EchavezDocument11 paginiHISTORY # 1 - PCGH, EchavezHynne Jhea EchavezÎncă nu există evaluări
- Enterobiasis CaseDocument4 paginiEnterobiasis CaseKimm Delos ReyesÎncă nu există evaluări
- CaseDocument2 paginiCaseJim Christian EllaserÎncă nu există evaluări
- Week 3 Case - DOBDocument3 paginiWeek 3 Case - DOBKirk Matthew ZhuÎncă nu există evaluări
- History: O Identifying DataDocument10 paginiHistory: O Identifying DataJofen Ann Hisoler TangpuzÎncă nu există evaluări
- Surg Week 4Document75 paginiSurg Week 4Casey YanoÎncă nu există evaluări
- Geri SOAPsampleDocument8 paginiGeri SOAPsampleJacquelineÎncă nu există evaluări
- IM-Generalized Peritonitis HX PEDocument20 paginiIM-Generalized Peritonitis HX PETrisÎncă nu există evaluări
- Protocol - IM Intermittent Fever, Epi Pain, HematuriaDocument4 paginiProtocol - IM Intermittent Fever, Epi Pain, HematuriaTrisÎncă nu există evaluări
- Thalassemia Report Edited2Document121 paginiThalassemia Report Edited2rjcarlos_05Încă nu există evaluări
- Hypertension Case IMDocument5 paginiHypertension Case IMPerlyn Mac Basiloy - AloÎncă nu există evaluări
- Case Protocol - GBS - TanguilanDocument7 paginiCase Protocol - GBS - TanguilanRosealie TanguilanÎncă nu există evaluări
- Highest Blood Pressure Was 140/90 MMHGDocument5 paginiHighest Blood Pressure Was 140/90 MMHGFG ArciagaÎncă nu există evaluări
- Pedia August 29Document4 paginiPedia August 29Raymund AldabaÎncă nu există evaluări
- Ent Case Report Acute Otitis Media Stage IIIDocument12 paginiEnt Case Report Acute Otitis Media Stage IIIRem Alfelor100% (1)
- Medical Report - PneumoniaeDocument8 paginiMedical Report - Pneumoniaenguyenhoavanchi2002Încă nu există evaluări
- Im - TBDocument11 paginiIm - TBTrisÎncă nu există evaluări
- De La Salle University Medical Center Department of Obstetrics and GynecologyDocument3 paginiDe La Salle University Medical Center Department of Obstetrics and GynecologyNehemiah FranciscoÎncă nu există evaluări
- Case Report 1Document12 paginiCase Report 1mike sharewÎncă nu există evaluări
- CASE STUDY Lung Ca With Pleural EffDocument8 paginiCASE STUDY Lung Ca With Pleural EffL4 CLERK - UY, Rhea Andrea F.Încă nu există evaluări
- Batmc OrthoDocument5 paginiBatmc OrthoDorish Faith CarilloÎncă nu există evaluări
- Sample Case ProtocolDocument6 paginiSample Case ProtocoljheyfteeÎncă nu există evaluări
- Soap Note TemplateDocument4 paginiSoap Note TemplateAdamÎncă nu există evaluări
- CPC CaseDocument8 paginiCPC CasePingky khingthongÎncă nu există evaluări
- General Data EdwinDocument3 paginiGeneral Data EdwinEdwin AngelesÎncă nu există evaluări
- Carbuncle, Incision, Drainage, DebridementDocument11 paginiCarbuncle, Incision, Drainage, DebridementAlvin Germo PasuquinÎncă nu există evaluări
- Bedside Rounds ZCMC Ward 8: History Taking and Physical ExaminationDocument28 paginiBedside Rounds ZCMC Ward 8: History Taking and Physical ExaminationneilaldentanÎncă nu există evaluări
- SOAP Note 1 - Breast CADocument4 paginiSOAP Note 1 - Breast CAacvalvarioÎncă nu există evaluări
- Acute AppendicitisDocument14 paginiAcute AppendicitisJane GarciaÎncă nu există evaluări
- Case Presentation Acute GlomerulonephritisDocument10 paginiCase Presentation Acute Glomerulonephritisminangsung minangnengÎncă nu există evaluări
- Started His Hearted Any CivillyDocument2 paginiStarted His Hearted Any CivillyEdsonnSPBrÎncă nu există evaluări
- Antonio Capacio PDFDocument1 paginăAntonio Capacio PDFIzzyMaxinoÎncă nu există evaluări
- Wipo Ip Ai 2 Ge 20 1Document9 paginiWipo Ip Ai 2 Ge 20 1IzzyMaxinoÎncă nu există evaluări
- Justice Teresita Leonardo-De Castro Cases (2008-2015) : Scope and Limitations of Taxation (Constitutional Limitations)Document4 paginiJustice Teresita Leonardo-De Castro Cases (2008-2015) : Scope and Limitations of Taxation (Constitutional Limitations)jimÎncă nu există evaluări
- Immune ChartDocument1 paginăImmune ChartIzzyMaxinoÎncă nu există evaluări
- The 7 Arpeggios From C Major PDFDocument4 paginiThe 7 Arpeggios From C Major PDFIzzyMaxinoÎncă nu există evaluări
- QDocument2 paginiQIzzyMaxinoÎncă nu există evaluări
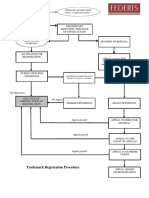
- Trademark Registration Procedure Flow ChartDocument1 paginăTrademark Registration Procedure Flow ChartIzzyMaxinoÎncă nu există evaluări
- 2011 NLRC Rules of Procedure Eb 11-12Document7 pagini2011 NLRC Rules of Procedure Eb 11-12hobbesianstudentÎncă nu există evaluări
- Affidavit of Graduating Candidate For USCDocument1 paginăAffidavit of Graduating Candidate For USCMamerto Egargo Jr.Încă nu există evaluări
- Aff of LossDocument1 paginăAff of LossIzzyMaxinoÎncă nu există evaluări
- D10P3B1S2019 5Document1 paginăD10P3B1S2019 5IzzyMaxinoÎncă nu există evaluări
- Drawing PDFDocument1 paginăDrawing PDFIzzyMaxinoÎncă nu există evaluări
- All About SuccessionDocument12 paginiAll About SuccessionIzzyMaxinoÎncă nu există evaluări
- Property Relations Between Husband and WifeDocument2 paginiProperty Relations Between Husband and WifeIzzyMaxino100% (1)
- Trade Secret in The PHDocument4 paginiTrade Secret in The PHIzzyMaxinoÎncă nu există evaluări
- Scanning ScriptsDocument3 paginiScanning ScriptsIzzyMaxinoÎncă nu există evaluări
- Felonies RPCDocument10 paginiFelonies RPCRouter JohnsonÎncă nu există evaluări
- Epoch Lavender PIPDocument2 paginiEpoch Lavender PIPIzzyMaxinoÎncă nu există evaluări
- AbcdDocument2 paginiAbcdIzzyMaxinoÎncă nu există evaluări
- 123Document2 pagini123IzzyMaxinoÎncă nu există evaluări
- OCA Circular No. 129 2009Document2 paginiOCA Circular No. 129 2009IzzyMaxinoÎncă nu există evaluări
- Q2019-TL-RZ7AEE: Pasig Branch Taguig Branch Cebu Branch Davao BranchDocument1 paginăQ2019-TL-RZ7AEE: Pasig Branch Taguig Branch Cebu Branch Davao BranchIzzyMaxinoÎncă nu există evaluări
- Billups Effective TeamDocument1 paginăBillups Effective TeamIzzyMaxinoÎncă nu există evaluări
- Rani Ti DineDocument2 paginiRani Ti Dinejordan11111111Încă nu există evaluări
- Longrich Product CatalogueDocument32 paginiLongrich Product CatalogueNeba Brandon.Încă nu există evaluări
- H. PyloriDocument13 paginiH. Pylorielene nikoleishviliÎncă nu există evaluări
- Metaplastic (Chronic) Atrophic Gastritis - UpToDate PDFDocument16 paginiMetaplastic (Chronic) Atrophic Gastritis - UpToDate PDFDinaÎncă nu există evaluări
- Ministry of Health of UkraineDocument31 paginiMinistry of Health of UkraineKhaled AbdoÎncă nu există evaluări
- An Unusual Case of Nonsurgical Pneumoperitoneum in A Pediatric P 2023 BurnsDocument5 paginiAn Unusual Case of Nonsurgical Pneumoperitoneum in A Pediatric P 2023 BurnsAdrian MoralesÎncă nu există evaluări
- Miwa 2016Document13 paginiMiwa 2016asri nurul ismiÎncă nu există evaluări
- Drug StudyDocument8 paginiDrug StudyjovanneyÎncă nu există evaluări
- Diabetic Foot Care: ReviewDocument7 paginiDiabetic Foot Care: ReviewRavi HardjumadyÎncă nu există evaluări
- Intestinal MetaplasiaDocument12 paginiIntestinal MetaplasiaarifÎncă nu există evaluări
- Gastroentrology LastDocument48 paginiGastroentrology LastAbdallah K. RamadanÎncă nu există evaluări
- AINS CaseDocument11 paginiAINS CaseMarilena TarcaÎncă nu există evaluări
- Lansoprazole 2Document1 paginăLansoprazole 2Ilham AchtzehnÎncă nu există evaluări
- Gastric FluidDocument33 paginiGastric FluidJaellah MatawaÎncă nu există evaluări
- Assessment of Digestive and Intestinal Tracts Disorders HAMDALLAHDocument141 paginiAssessment of Digestive and Intestinal Tracts Disorders HAMDALLAHMAYHAMDALLAHÎncă nu există evaluări
- Epigastric Pain (Up Date) Masroel GontarDocument52 paginiEpigastric Pain (Up Date) Masroel GontarTaufik Akbar Faried Lubis50% (2)
- Gastric Antral Perf in 15 Yr BoyDocument29 paginiGastric Antral Perf in 15 Yr BoyRajesh MenonÎncă nu există evaluări
- Medscape GastritisDocument13 paginiMedscape GastritisFalaudin LaksanaÎncă nu există evaluări
- (HLMN 4-15) Approach To The Adult With Dyspepsia - UpToDateDocument18 pagini(HLMN 4-15) Approach To The Adult With Dyspepsia - UpToDateandylumanÎncă nu există evaluări
- Gastric Outlet Obstruction: BY: Tharun Balaji Vinay GautamDocument19 paginiGastric Outlet Obstruction: BY: Tharun Balaji Vinay Gautam7hhdfc8vmwÎncă nu există evaluări
- Welcome To TampcolDocument5 paginiWelcome To TampcolmurugangdÎncă nu există evaluări
- Omeprazole PDFDocument8 paginiOmeprazole PDFRafael SyfuÎncă nu există evaluări