S-ar putea să vă placă și
- International Survey Reveals Differences in Managing Infections and Preterm BirthDocument6 paginiInternational Survey Reveals Differences in Managing Infections and Preterm BirthKhazoliyaÎncă nu există evaluări
- H PyloriDocument8 paginiH PyloriHabtamu WondifrawÎncă nu există evaluări
- Jurnal Reading 3Document9 paginiJurnal Reading 3Harmas Novryan FarezaÎncă nu există evaluări
- Epidemiological Profile of Helicobacter Pylori Infection AlgeriaDocument5 paginiEpidemiological Profile of Helicobacter Pylori Infection AlgeriaAhmad AliÎncă nu există evaluări
- Journal Reading Pediatric TuberculosaDocument22 paginiJournal Reading Pediatric TuberculosaRicky ApriliandoÎncă nu există evaluări
- Clinical and Endoscopic Findings in Children WithDocument6 paginiClinical and Endoscopic Findings in Children WithzikraalfaÎncă nu există evaluări
- Journal PNTD 0007809 PDFDocument21 paginiJournal PNTD 0007809 PDFRegele BrânzăÎncă nu există evaluări
- Typhoid Fever in Children in Africa : ViewpointDocument9 paginiTyphoid Fever in Children in Africa : ViewpointFaiz Yunanto MangoendiprodjoÎncă nu există evaluări
- Introduction to Community Acquired Pneumonia in ChildrenDocument7 paginiIntroduction to Community Acquired Pneumonia in ChildrenindahÎncă nu există evaluări
- Fritzell2018 PDFDocument29 paginiFritzell2018 PDFJuan Fernando BermúdezÎncă nu există evaluări
- Annals of Medicine and Surgery: SciencedirectDocument5 paginiAnnals of Medicine and Surgery: SciencedirectSantos Pardo GomezÎncă nu există evaluări
- Review 1Document23 paginiReview 1ms. chokyuÎncă nu există evaluări
- Epidemiological Risk Factors For Adult Dengue in Singapore: An 8-Year Nested Test Negative Case Control StudyDocument9 paginiEpidemiological Risk Factors For Adult Dengue in Singapore: An 8-Year Nested Test Negative Case Control StudydouwesdÎncă nu există evaluări
- WJG 18 4335Document7 paginiWJG 18 4335aalmadasalazarÎncă nu există evaluări
- Current State-Of-The-Art Diagnostics For Norovirus Detection - Model Approaches For Point-Of-Care AnalysisDocument12 paginiCurrent State-Of-The-Art Diagnostics For Norovirus Detection - Model Approaches For Point-Of-Care AnalysisRayhan OpuÎncă nu există evaluări
- Intestinal Parasitic Infections and Associated Factors Among People Living With HIV/AIDS in Ethiopia: A Systematic Review and Meta AnalysiDocument17 paginiIntestinal Parasitic Infections and Associated Factors Among People Living With HIV/AIDS in Ethiopia: A Systematic Review and Meta AnalysiminiwhiteyÎncă nu există evaluări
- Diagnostic Analysis For TB: A Comparative Study Between Bacilloscopy, Culture and PCR (Gene-Xpert) TechniquesDocument6 paginiDiagnostic Analysis For TB: A Comparative Study Between Bacilloscopy, Culture and PCR (Gene-Xpert) TechniquesIJAERS JOURNALÎncă nu există evaluări
- Clinical Value of Serology For The Diagnosis of Strongyloidiasis in Travelers and Migrants - A 4-Year Retrospective Study Using The Bordier IVD Strongyloides Ratti ELISA AssayDocument10 paginiClinical Value of Serology For The Diagnosis of Strongyloidiasis in Travelers and Migrants - A 4-Year Retrospective Study Using The Bordier IVD Strongyloides Ratti ELISA Assaygwyneth.green.512Încă nu există evaluări
- Increasing Smear Positive Tuberculosis Detection Using A Clinical ScoreDocument8 paginiIncreasing Smear Positive Tuberculosis Detection Using A Clinical ScoreMezgebu Yitayal MengistuÎncă nu există evaluări
- Use and Quality of Point-Of-Care Microscopy Urine Culture and Susceptibility Testing For Urinalysis in General PracticeDocument9 paginiUse and Quality of Point-Of-Care Microscopy Urine Culture and Susceptibility Testing For Urinalysis in General Practicemicrobehunter007Încă nu există evaluări
- JPID - Traqueíte Bacteriana Revisão - 2009Document12 paginiJPID - Traqueíte Bacteriana Revisão - 2009Juliana MeirelesÎncă nu există evaluări
- s42269 021 00597 9Document7 paginis42269 021 00597 9Thrilling MahediÎncă nu există evaluări
- 139683-Article Text-372650-1-10-20160718Document9 pagini139683-Article Text-372650-1-10-20160718MATTHEW JALOWE MACARANASÎncă nu există evaluări
- Helicobacter - 2016 - Leja - Epidemiology of Helicobacter Pylori InfectionDocument5 paginiHelicobacter - 2016 - Leja - Epidemiology of Helicobacter Pylori InfectionmukwayasadikÎncă nu există evaluări
- Early diagnosis and treatment of childhood tuberculosisDocument12 paginiEarly diagnosis and treatment of childhood tuberculosisPaomo Zhixia EarlyÎncă nu există evaluări
- TB HivDocument6 paginiTB HivIwuohaEjiroÎncă nu există evaluări
- Title Use of Fibreoptic Bronchoscopy in Diagnosing Sputum Smear-Negative Pulmonary TuberculosisDocument46 paginiTitle Use of Fibreoptic Bronchoscopy in Diagnosing Sputum Smear-Negative Pulmonary TuberculosisHam FGÎncă nu există evaluări
- Group - 6 Research MEthodologyDocument19 paginiGroup - 6 Research MEthodologyN GullÎncă nu există evaluări
- Rapid Diagnosis of Diarrhea Caused by Shigella Sonnei Using Dipsticks Comparison of Rectal Swabs, Direct Stool and Stool CultureDocument9 paginiRapid Diagnosis of Diarrhea Caused by Shigella Sonnei Using Dipsticks Comparison of Rectal Swabs, Direct Stool and Stool CultureSuci IrianiÎncă nu există evaluări
- Gastroenteritis in Childhood A Retrospective StudyDocument8 paginiGastroenteritis in Childhood A Retrospective StudyTiara Sekar AyudhipashaÎncă nu există evaluări
- 17akinbolaji EtalDocument5 pagini17akinbolaji EtaleditorijmrhsÎncă nu există evaluări
- Abebe 2010Document7 paginiAbebe 2010Ricardo Ivan Vertiz OsoresÎncă nu există evaluări
- Art GEBADocument8 paginiArt GEBAJhonathan Andres Garcia FiallosÎncă nu există evaluări
- Art:10.1186/1756 3305 6 3Document8 paginiArt:10.1186/1756 3305 6 3Bagus Muhammad IhsanÎncă nu există evaluări
- Abdominal Tuberculosis Clinical Profile And.11Document7 paginiAbdominal Tuberculosis Clinical Profile And.11Yutenji NaritaÎncă nu există evaluări
- HHS Public AccessDocument22 paginiHHS Public AccessZakirÎncă nu există evaluări
- 67 1437543936 PDFDocument5 pagini67 1437543936 PDFrivandiÎncă nu există evaluări
- Efficiency of Web Application and Spaced Repetition Algorithms As An Aid in Preparing To Practical Examination of HistologyDocument2 paginiEfficiency of Web Application and Spaced Repetition Algorithms As An Aid in Preparing To Practical Examination of HistologyduffuchimpsÎncă nu există evaluări
- Bordetella Pertussis in Sporadic and Outbreak Settings in Alberta, Canada, July 2004 - December 2012Document9 paginiBordetella Pertussis in Sporadic and Outbreak Settings in Alberta, Canada, July 2004 - December 2012Kambang SariadjiÎncă nu există evaluări
- Prevalence, Incidence and Risk Factors For Helicobacter Pylori Infection in A Cohort of Portuguese Adolescents (Epiteen)Document6 paginiPrevalence, Incidence and Risk Factors For Helicobacter Pylori Infection in A Cohort of Portuguese Adolescents (Epiteen)yundaÎncă nu există evaluări
- Research Article: Viral Agents of Diarrhea in Young Children in Two Primary Health Centers in Edo State, NigeriaDocument6 paginiResearch Article: Viral Agents of Diarrhea in Young Children in Two Primary Health Centers in Edo State, NigeriariniÎncă nu există evaluări
- Prevalence and Determinants of Human Immunodeficiency Virus and Tuberculosis Co-Infection at Kampala International University Teaching HospitalDocument6 paginiPrevalence and Determinants of Human Immunodeficiency Virus and Tuberculosis Co-Infection at Kampala International University Teaching HospitalKIU PUBLICATION AND EXTENSIONÎncă nu există evaluări
- The Aetiology and Antibiotic Management of Community-Acquired Pneumonia in Adults in Europe: A Literature ReviewDocument15 paginiThe Aetiology and Antibiotic Management of Community-Acquired Pneumonia in Adults in Europe: A Literature ReviewPutu Sukma RadhanaÎncă nu există evaluări
- Suspected Urinary Tract Infection in Primary Care, DenmarkDocument6 paginiSuspected Urinary Tract Infection in Primary Care, DenmarkImelda Nafa PawestriÎncă nu există evaluări
- International Journal of Infectious Diseases: SciencedirectDocument8 paginiInternational Journal of Infectious Diseases: SciencedirectMada Pasalli SaludungÎncă nu există evaluări
- Research Journal4Document5 paginiResearch Journal4Jayhan AmbrocioÎncă nu există evaluări
- H Pylori Ricci2007 PDFDocument15 paginiH Pylori Ricci2007 PDFHasbiallah YusufÎncă nu există evaluări
- Erj Pleural TBDocument9 paginiErj Pleural TBmalleshmadeshÎncă nu există evaluări
- 6 Ijmpsjun20196Document6 pagini6 Ijmpsjun20196TJPRC PublicationsÎncă nu există evaluări
- Global H Pylori DataDocument10 paginiGlobal H Pylori DataSohail ManzoorÎncă nu există evaluări
- Abcesele FicatuluiDocument4 paginiAbcesele FicatuluiMihaela AlinaÎncă nu există evaluări
- Petersen 2001Document30 paginiPetersen 2001Bianca MagnelliÎncă nu există evaluări
- Microbial causes of acute diarrhoea in Sudanese childrenDocument6 paginiMicrobial causes of acute diarrhoea in Sudanese childrenandani delabeneÎncă nu există evaluări
- Ultrasound findings in dengue fever patientsDocument4 paginiUltrasound findings in dengue fever patientsSubhan Hasbi YudaÎncă nu există evaluări
- Helicobacter Pylori Infection - Recent Developments in DiagnosisDocument16 paginiHelicobacter Pylori Infection - Recent Developments in DiagnosisRima Carolina Bahsas ZakyÎncă nu există evaluări
- Diagnosis & Treatment of Tuberculosis in HIV Co-Infected PatientsDocument16 paginiDiagnosis & Treatment of Tuberculosis in HIV Co-Infected PatientsdevisilalahiÎncă nu există evaluări
- Paper RespiratorioDocument8 paginiPaper RespiratorioDave IgnacioÎncă nu există evaluări
- Fever of Unknown OriginDocument6 paginiFever of Unknown OriginfebifebriantyÎncă nu există evaluări
- Drug Resistance in Mycobacterium Tuberculosis PDFDocument18 paginiDrug Resistance in Mycobacterium Tuberculosis PDFMuhammad Addinul HudaÎncă nu există evaluări
- Colitis: A Practical Approach to Colon and Ileum Biopsy InterpretationDe la EverandColitis: A Practical Approach to Colon and Ileum Biopsy InterpretationAnne Jouret-MourinÎncă nu există evaluări
- Fetal Heart Defects and Measures of Cerebral Size: Objectives Study DesignDocument8 paginiFetal Heart Defects and Measures of Cerebral Size: Objectives Study DesignAdrian KhomanÎncă nu există evaluări
- 10 1002@ppul 1950160309 PDFDocument13 pagini10 1002@ppul 1950160309 PDFAdrian KhomanÎncă nu există evaluări
- Chronic Lung Disease in Premature BabiesDocument2 paginiChronic Lung Disease in Premature BabiesAdrian KhomanÎncă nu există evaluări
- BLT 15 259Document9 paginiBLT 15 259Adrian KhomanÎncă nu există evaluări
- Danne 2018Document54 paginiDanne 2018Adrian KhomanÎncă nu există evaluări
- Chronic Lung Disease in Premature BabiesDocument2 paginiChronic Lung Disease in Premature BabiesAdrian KhomanÎncă nu există evaluări
- Jurnal Neuroo Wanigasinghe2015Document7 paginiJurnal Neuroo Wanigasinghe2015melly adityaÎncă nu există evaluări
- Be Rent Sen 2015Document12 paginiBe Rent Sen 2015Adrian KhomanÎncă nu există evaluări
- DHF Menurut WHO 2011Document212 paginiDHF Menurut WHO 2011Jamal SutrisnaÎncă nu există evaluări
- Kugelman2007 PDFDocument7 paginiKugelman2007 PDFAdrian KhomanÎncă nu există evaluări
- Merrill 2004Document9 paginiMerrill 2004Adrian KhomanÎncă nu există evaluări
- Be Rent Sen 2015Document12 paginiBe Rent Sen 2015Adrian KhomanÎncă nu există evaluări
- Miaoying Zhang, Xiaojing Li, Li Xi, Zhuhui Zhao, Ruoqian Cheng, Bingbing Wu and Feihong LuoDocument1 paginăMiaoying Zhang, Xiaojing Li, Li Xi, Zhuhui Zhao, Ruoqian Cheng, Bingbing Wu and Feihong LuoAdrian KhomanÎncă nu există evaluări
- Jae 201174012905Document5 paginiJae 201174012905Adrian KhomanÎncă nu există evaluări
- Practical Algorithms in Pediatric Hematology and OncologyDocument119 paginiPractical Algorithms in Pediatric Hematology and OncologyNubia Ahumadaa100% (5)
- United States Patent (19) 11 Patent Number: 5,969,606: Reber Et Al. (45) Date of Patent: Oct. 19, 1999Document12 paginiUnited States Patent (19) 11 Patent Number: 5,969,606: Reber Et Al. (45) Date of Patent: Oct. 19, 1999Adrian KhomanÎncă nu există evaluări
- New Newstart 2Document1 paginăNew Newstart 2Adrian KhomanÎncă nu există evaluări
- Alan Sari 2016Document11 paginiAlan Sari 2016Adrian KhomanÎncă nu există evaluări
- Ehz 467Document65 paginiEhz 467Coy Calapatia-TorresÎncă nu există evaluări
- Status Nutrisi WHO Laki-LakiDocument1 paginăStatus Nutrisi WHO Laki-LakiAdrian KhomanÎncă nu există evaluări
- Treatment of Autoimmune Hemolytic Anemias, 2014 ReviewDocument8 paginiTreatment of Autoimmune Hemolytic Anemias, 2014 ReviewSabina UlubeanuÎncă nu există evaluări
- Pocket Pediatrics Handbook for Children by MGHDocument5 paginiPocket Pediatrics Handbook for Children by MGHAdrian KhomanÎncă nu există evaluări
- Pediatric Cardiology: Original ArticlesDocument5 paginiPediatric Cardiology: Original ArticlesAdrian KhomanÎncă nu există evaluări
- Hemodynamic Study: O Content (mL/100 ML) HB × 1.36 × (O Sat/100)Document9 paginiHemodynamic Study: O Content (mL/100 ML) HB × 1.36 × (O Sat/100)Adrian KhomanÎncă nu există evaluări
- Treatment of Autoimmune Hemolytic Anemias, 2014 ReviewDocument8 paginiTreatment of Autoimmune Hemolytic Anemias, 2014 ReviewSabina UlubeanuÎncă nu există evaluări
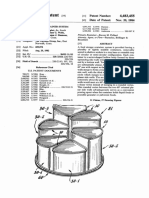
- Food storage container system patentDocument13 paginiFood storage container system patentAdrian KhomanÎncă nu există evaluări
- Diagnostic and Therapeutic Challenges of Primary Autoimmune Haemolytic Anaemia in ChildrenDocument7 paginiDiagnostic and Therapeutic Challenges of Primary Autoimmune Haemolytic Anaemia in ChildrenAdrian KhomanÎncă nu există evaluări
- Breastfeeding Rates and Programs in Europe: A Survey of 11 National Breastfeeding Committees and RepresentativesDocument8 paginiBreastfeeding Rates and Programs in Europe: A Survey of 11 National Breastfeeding Committees and RepresentativesAdrian KhomanÎncă nu există evaluări
- United States Patent (19) 11 Patent Number: 5,969,606: Reber Et Al. (45) Date of Patent: Oct. 19, 1999Document12 paginiUnited States Patent (19) 11 Patent Number: 5,969,606: Reber Et Al. (45) Date of Patent: Oct. 19, 1999Adrian KhomanÎncă nu există evaluări
- Pediatric Neurology: Hye-Ryun Yeh MD, Min-Jee Kim MD, Tae-Sung Ko MD, PHD, Mi-Sun Yum MD, PHD, Su-Jeong You MD, PHDDocument6 paginiPediatric Neurology: Hye-Ryun Yeh MD, Min-Jee Kim MD, Tae-Sung Ko MD, PHD, Mi-Sun Yum MD, PHD, Su-Jeong You MD, PHDAdrian KhomanÎncă nu există evaluări
- Role of MicrofinanceDocument1 paginăRole of MicrofinanceuttamsudhirÎncă nu există evaluări
- 2021.01 - Key-Findings - Green Bond Premium - ENDocument6 pagini2021.01 - Key-Findings - Green Bond Premium - ENlypozÎncă nu există evaluări
- Plastic BanDocument3 paginiPlastic BanSangeetha IlangoÎncă nu există evaluări
- The Muscle and Strength Training Pyramid v2.0 Training by Eric Helms-9Document31 paginiThe Muscle and Strength Training Pyramid v2.0 Training by Eric Helms-9Hamada MansourÎncă nu există evaluări
- Environment Health: European Research OnDocument73 paginiEnvironment Health: European Research OnDaiuk.DakÎncă nu există evaluări
- MGN 363Document14 paginiMGN 363Nitin PatidarÎncă nu există evaluări
- Chapter 3 Theoretical ConsiderationsDocument8 paginiChapter 3 Theoretical Considerationsapi-3696675Încă nu există evaluări
- Ball Bearings 1Document17 paginiBall Bearings 1ManicharanÎncă nu există evaluări
- Martek Navgard BnwasDocument4 paginiMartek Navgard BnwasСергей БородинÎncă nu există evaluări
- User Manual With FAQs - Sales Invoice For Petrol PumpsDocument10 paginiUser Manual With FAQs - Sales Invoice For Petrol PumpsRavindra MittalÎncă nu există evaluări
- Saturn Engine Compression Test GuideDocument7 paginiSaturn Engine Compression Test GuideManuel IzquierdoÎncă nu există evaluări
- An Overview of Radar Cross Section Measurement Techniques: Airplanes AIRDocument3 paginiAn Overview of Radar Cross Section Measurement Techniques: Airplanes AIRiamnbroneÎncă nu există evaluări
- Railway noise source modeling and measurement methodsDocument78 paginiRailway noise source modeling and measurement methodsftyoneyamaÎncă nu există evaluări
- 7-Seater MPV: Kia SingaporeDocument16 pagini7-Seater MPV: Kia SingaporeadiÎncă nu există evaluări
- Praveen Verma Auto CAD IntershipDocument15 paginiPraveen Verma Auto CAD IntershipPraveen vermaÎncă nu există evaluări
- 10 Questions About Independent ReadingDocument4 pagini10 Questions About Independent ReadingdewiÎncă nu există evaluări
- Product Placement in Movies- Impact on SalesDocument3 paginiProduct Placement in Movies- Impact on SalesBhavya DiddeeÎncă nu există evaluări
- Hepatobiliary Surgery BlumgartDocument301 paginiHepatobiliary Surgery Blumgartaejazahsan100% (7)
- Case Study Series by Afterschoool - The Great Hotels of BikanerDocument24 paginiCase Study Series by Afterschoool - The Great Hotels of BikanerKNOWLEDGE CREATORSÎncă nu există evaluări
- Ye Zindagi Aur Mujhe Fanaa KardeDocument9 paginiYe Zindagi Aur Mujhe Fanaa Kardeankur9359saxenaÎncă nu există evaluări
- Manual Cisco - DPC3925Document106 paginiManual Cisco - DPC3925HábnerTeixeiraCostaÎncă nu există evaluări
- AbolethDocument3 paginiAbolethjlewis_4Încă nu există evaluări
- Human Resource Planning and Corroporate Strategies: Meaning and Definition of StrategyDocument19 paginiHuman Resource Planning and Corroporate Strategies: Meaning and Definition of StrategyRashmi KhublaniÎncă nu există evaluări
- Consular Assistance For Indians Living Abroad Through "MADAD"Document12 paginiConsular Assistance For Indians Living Abroad Through "MADAD"NewsBharatiÎncă nu există evaluări
- The Barber of SevilleDocument1 paginăThe Barber of SevilleAine MulveyÎncă nu există evaluări
- Essential Components of an Effective Road Drainage SystemDocument11 paginiEssential Components of an Effective Road Drainage SystemRaisanAlcebarÎncă nu există evaluări
- The International Journal of Periodontics & Restorative DentistryDocument7 paginiThe International Journal of Periodontics & Restorative DentistrytaniaÎncă nu există evaluări
- Lecture Notes On Revaluation and Impairment PDFDocument6 paginiLecture Notes On Revaluation and Impairment PDFjudel ArielÎncă nu există evaluări
- Msme'S Premium Product Catalogue Book 2020: Craft CategoryDocument50 paginiMsme'S Premium Product Catalogue Book 2020: Craft CategoryTomikoVanÎncă nu există evaluări