S-ar putea să vă placă și
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- 1 s2.0 S0167844214000561 MainDocument10 pagini1 s2.0 S0167844214000561 MainArun KumarÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Souit 2016Document6 paginiSouit 2016Arun KumarÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- 2015 - Towards-a-Robotic-Knee-Exoskeleton-Control-Based-on-Human Intention Through EEG and sEMGsignalsDocument8 pagini2015 - Towards-a-Robotic-Knee-Exoskeleton-Control-Based-on-Human Intention Through EEG and sEMGsignalsArun KumarÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- 1999 - Evaluation of The Formula of Stress Intensity Factor Ki For Semi-Elliptical Surface CrackDocument4 pagini1999 - Evaluation of The Formula of Stress Intensity Factor Ki For Semi-Elliptical Surface CrackArun KumarÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Stress Intensity Factors of A Central Slant CrackDocument9 paginiStress Intensity Factors of A Central Slant CrackArun KumarÎncă nu există evaluări
- 1999 - Evaluation of The Stress Intensity Factor For Cracks in ElastomersDocument4 pagini1999 - Evaluation of The Stress Intensity Factor For Cracks in ElastomersArun KumarÎncă nu există evaluări
- 2004 - Cracks at Rounded V-Notch Tips An Analytical Expression For The Stress Intensity FactorDocument7 pagini2004 - Cracks at Rounded V-Notch Tips An Analytical Expression For The Stress Intensity FactorArun KumarÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- 2008 Failure of Refurbished Turbine Blades in A Power Station by Improper Heat TreatmentDocument6 pagini2008 Failure of Refurbished Turbine Blades in A Power Station by Improper Heat TreatmentArun KumarÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- 1999 - Finite Element Modelling of Fatigue Crack Growth of SurfaceDocument16 pagini1999 - Finite Element Modelling of Fatigue Crack Growth of SurfaceArun KumarÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- 1997 - Analytical and Experimental Determination of Dynamic ImpactDocument6 pagini1997 - Analytical and Experimental Determination of Dynamic ImpactArun KumarÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- 2002 - The Effect of A Plastically Deformed Zone Near Crack Tip On The Stress Intensity FactorsDocument6 pagini2002 - The Effect of A Plastically Deformed Zone Near Crack Tip On The Stress Intensity FactorsArun KumarÎncă nu există evaluări
- 2011 Damage Tolerant Design and Nondestructive InspectionDocument11 pagini2011 Damage Tolerant Design and Nondestructive InspectionArun KumarÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Talzat ZachariaDocument8 paginiTalzat ZachariaArun KumarÎncă nu există evaluări
- Biology 09 00399 1Document14 paginiBiology 09 00399 1Arun KumarÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Computers 11 00113 v2Document21 paginiComputers 11 00113 v2Arun KumarÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- 04.2003.sustainable Product Development and Manufacturing by Considering Environmental RequirementsDocument8 pagini04.2003.sustainable Product Development and Manufacturing by Considering Environmental RequirementsArun KumarÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Online Final OrderDocument3 paginiOnline Final OrderArun KumarÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Ijsi 09 2012 0022Document22 paginiIjsi 09 2012 0022Arun KumarÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- 2019 AbbDocument10 pagini2019 AbbArun KumarÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- How To Connect Campus VPN With A Client App: Information and Communication Technology ServicesDocument2 paginiHow To Connect Campus VPN With A Client App: Information and Communication Technology ServicesArun KumarÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- .2014 - A Review Paper On Pressure Vessel Design and AnalysisDocument7 pagini.2014 - A Review Paper On Pressure Vessel Design and AnalysisArun KumarÎncă nu există evaluări
- Talzat Zacharia PDFDocument16 paginiTalzat Zacharia PDFArun KumarÎncă nu există evaluări
- 1997 - Relationship Between CTOD and J For Stationary and Growing CracksDocument13 pagini1997 - Relationship Between CTOD and J For Stationary and Growing CracksArun KumarÎncă nu există evaluări
- A Brief Guide To Calculating Embodied CarbonDocument6 paginiA Brief Guide To Calculating Embodied Carbonmatt calvertÎncă nu există evaluări
- ISRO Scientist Engineer Civil Paper 7 January 2024Document31 paginiISRO Scientist Engineer Civil Paper 7 January 2024SATHISH KUMAR SÎncă nu există evaluări
- FINAL SIP PRINT OUT Guransh 7sepDocument58 paginiFINAL SIP PRINT OUT Guransh 7sepAmbuj Roy100% (1)
- Royal Continental, Niger Project - Pi - 3751Document9 paginiRoyal Continental, Niger Project - Pi - 3751ashishvaidÎncă nu există evaluări
- Poly - Mer: Cartoon Schematic of Polymer MoleculesDocument7 paginiPoly - Mer: Cartoon Schematic of Polymer MoleculesElenaDiSavoiaÎncă nu există evaluări
- Chemistry For Engineers: Assignment 1Document4 paginiChemistry For Engineers: Assignment 1Thanh Tan PhamÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Determination of In-Situ Unit Weight of Soil: Experiment No 2 & 3 Soil Mechanics Laboratory CE PC 594Document30 paginiDetermination of In-Situ Unit Weight of Soil: Experiment No 2 & 3 Soil Mechanics Laboratory CE PC 594SumanHaldar100% (1)
- Drawing & Catalogue-Kumwell PDFDocument15 paginiDrawing & Catalogue-Kumwell PDFDevis RipomoÎncă nu există evaluări
- Load-Bearing Glass Structures PDFDocument16 paginiLoad-Bearing Glass Structures PDFbatteekhÎncă nu există evaluări
- Test Bank The Human Body Health Illness 5th Edition HerlihyDocument15 paginiTest Bank The Human Body Health Illness 5th Edition HerlihyRhonda Mosholder100% (22)
- Doubly Reinforced Beams: Tension and Compression Steel Both YieldingDocument24 paginiDoubly Reinforced Beams: Tension and Compression Steel Both Yieldingمحمد بركاتÎncă nu există evaluări
- 50CDocument6 pagini50Cjhacademyhyd89% (9)
- Deltech DK60 and AboveDocument4 paginiDeltech DK60 and Abovesales-admin.bdgÎncă nu există evaluări
- AVL Internal Manufacturer 191097Document285 paginiAVL Internal Manufacturer 191097Seyyed Amir MohmmadiÎncă nu există evaluări
- A Comparison of PH Eur and DSP RequirementsDocument4 paginiA Comparison of PH Eur and DSP RequirementsAyoub TofixÎncă nu există evaluări
- ExerciseDocument4 paginiExerciseAshebirÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Wiring Cable StandardDocument6 paginiWiring Cable StandardAli AhmadÎncă nu există evaluări
- Unit SS Design Calculations For PrecastDocument13 paginiUnit SS Design Calculations For PrecastKumar SureshÎncă nu există evaluări
- Yield Strength Yield Point Stress Yield Point Stress Elastic Limit Elastic LimitDocument1 paginăYield Strength Yield Point Stress Yield Point Stress Elastic Limit Elastic LimitCarlito Jr JavilloÎncă nu există evaluări
- Fiber Reinforced Plastics VesselsDocument5 paginiFiber Reinforced Plastics VesselsandreshuelvaÎncă nu există evaluări
- Gate 2004Document8 paginiGate 2004Shailendra Mishra100% (1)
- Balancing Word Equations PracticeDocument3 paginiBalancing Word Equations PracticemmÎncă nu există evaluări
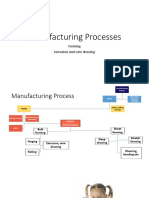
- Slide 11 Extrusion and Wire DrawingDocument53 paginiSlide 11 Extrusion and Wire Drawingjohn doeÎncă nu există evaluări
- NMR Solvents - Unsurpassed Quality For Peak PerformanceDocument12 paginiNMR Solvents - Unsurpassed Quality For Peak PerformanceSigma-Aldrich100% (1)
- Pre-Final Bill Supplimentary works-MVGR 02.07.2019Document112 paginiPre-Final Bill Supplimentary works-MVGR 02.07.2019Anonymous ImoZI0363Încă nu există evaluări
- CHEM181.Experiment 8 DetermiantionofDissolvedOxygenDocument5 paginiCHEM181.Experiment 8 DetermiantionofDissolvedOxygenDenampo Ivan MikhaelÎncă nu există evaluări
- Material TestingDocument35 paginiMaterial TestinghanyÎncă nu există evaluări
- Phase Equilibrium Study in The CaODocument5 paginiPhase Equilibrium Study in The CaOsattiricÎncă nu există evaluări
- Science Paper 3 - SolvedDocument10 paginiScience Paper 3 - SolvedRavi KumarÎncă nu există evaluări
- Common SSR For The Year 2019-20 (For All AP Power Utilities)Document48 paginiCommon SSR For The Year 2019-20 (For All AP Power Utilities)SIVA NAGA SUDHEER SIDDANIÎncă nu există evaluări
- Guidelines for Chemical Process Quantitative Risk AnalysisDe la EverandGuidelines for Chemical Process Quantitative Risk AnalysisEvaluare: 5 din 5 stele5/5 (1)
- Sodium Bicarbonate: Nature's Unique First Aid RemedyDe la EverandSodium Bicarbonate: Nature's Unique First Aid RemedyEvaluare: 5 din 5 stele5/5 (21)
- Lees' Process Safety Essentials: Hazard Identification, Assessment and ControlDe la EverandLees' Process Safety Essentials: Hazard Identification, Assessment and ControlEvaluare: 4 din 5 stele4/5 (4)