S-ar putea să vă placă și
- Employer's Work Accident - Illness Report Form (DOLE - BWC - OHSD - IP-6) DocDocument1 paginăEmployer's Work Accident - Illness Report Form (DOLE - BWC - OHSD - IP-6) DocTsin Pajaro- Inocian100% (3)
- Wair Ip-6 PDFDocument2 paginiWair Ip-6 PDFJMÎncă nu există evaluări
- DOLE Annual Medical Report - Sample & GuideDocument5 paginiDOLE Annual Medical Report - Sample & Guidewindell Patalinghug57% (7)
- Annual Medical Report Form (DOLE - BWC - HSD - ) H-47-A)Document7 paginiAnnual Medical Report Form (DOLE - BWC - HSD - ) H-47-A)jaysonmalaa100% (2)
- Annual Medical ReportDocument6 paginiAnnual Medical ReportMark BuendiaÎncă nu există evaluări
- Safety and Health ProgramDocument12 paginiSafety and Health ProgramRichard Gabitan100% (2)
- Sample Report For Annual Health SafetyDocument2 paginiSample Report For Annual Health SafetyDian AvilaÎncă nu există evaluări
- Report of Safety and Health OrganizationDocument1 paginăReport of Safety and Health OrganizationМарк Артём Лимот АпаллаÎncă nu există evaluări
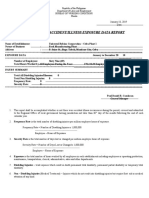
- Annual Work Accident/Illness Exposure Data Report: Dole/Bwc/Ohsd/Ip-6BDocument1 paginăAnnual Work Accident/Illness Exposure Data Report: Dole/Bwc/Ohsd/Ip-6BMark Buendia91% (11)
- OSH Program Template (RA 11058)Document11 paginiOSH Program Template (RA 11058)Rodeth MarquezÎncă nu există evaluări
- WAIR Employer's Work-Accident-Illness ReportDocument2 paginiWAIR Employer's Work-Accident-Illness ReportAlmario Sagun80% (5)
- RSO-Report On Health and Safety OrganizationDocument2 paginiRSO-Report On Health and Safety OrganizationAlaine Sobredo0% (1)
- Mental Health and Healthy Lifestyle Workplace Policy and ProgramDocument7 paginiMental Health and Healthy Lifestyle Workplace Policy and ProgramDarryl Robles100% (3)
- AEDR Annual Work Accident-Illness Exposure Data ReportDocument4 paginiAEDR Annual Work Accident-Illness Exposure Data ReportAlmario Sagun100% (1)
- Dole Safety CommitteeDocument4 paginiDole Safety CommitteeМарк Артём Лимот АпаллаÎncă nu există evaluări
- Salient Features of OSH LegislationsDocument28 paginiSalient Features of OSH LegislationsKhalied Noynay100% (1)
- Report of Safety and Health Organization MarilaoDocument1 paginăReport of Safety and Health Organization MarilaoМарк Артём Лимот АпаллаÎncă nu există evaluări
- Instructions On How To Properly Fill in The WAIRDocument17 paginiInstructions On How To Properly Fill in The WAIRLauro CanceranÎncă nu există evaluări
- Annual Medical Report Form (DOLE - BWC - HSD - ) H-47-A)Document7 paginiAnnual Medical Report Form (DOLE - BWC - HSD - ) H-47-A)Angelica Ponce100% (2)
- Template - Commitment To Comply With OSH RequirementsDocument1 paginăTemplate - Commitment To Comply With OSH RequirementsKaye Reyes67% (3)
- OSH Program SampleDocument9 paginiOSH Program SampleLeah Ann AquinoÎncă nu există evaluări
- Template OSHprogramDocument10 paginiTemplate OSHprogramRafael OcampoÎncă nu există evaluări
- Fire Brigade Organizational ChartDocument1 paginăFire Brigade Organizational ChartМарк Артём Лимот Апалла100% (2)
- DOLE OSH Program TemplateDocument13 paginiDOLE OSH Program Templateoshc caraga100% (1)
- TB Workplace Policy & ProgramDocument3 paginiTB Workplace Policy & Programraighnejames19100% (2)
- Sample Appointment Letter of Safety OfficerDocument2 paginiSample Appointment Letter of Safety OfficerAnonymous iu6zISy71% (24)
- OSH Program-New FormatDocument14 paginiOSH Program-New FormatJesson PulmanoÎncă nu există evaluări
- Dole OSH ProgramDocument10 paginiDole OSH Programpolar1030090% (1)
- Bosh Osh Program Template 11.11.2020Document13 paginiBosh Osh Program Template 11.11.2020Avelino Coballes IV0% (1)
- DOLE BWC OHSD IP 6bDocument1 paginăDOLE BWC OHSD IP 6bYurs100% (1)
- Appointment Letter With Duties and ResponsibilitiesDocument6 paginiAppointment Letter With Duties and ResponsibilitiesLenlen VelascoÎncă nu există evaluări
- SMR Sample With NotesDocument11 paginiSMR Sample With NotesTris100% (7)
- Dole BWC Ohsd Ip 5 Page 1Document2 paginiDole BWC Ohsd Ip 5 Page 1Yurs100% (1)
- PCO Request LetterDocument2 paginiPCO Request LetterAngelito Regulacion50% (2)
- TCC First MeetingDocument2 paginiTCC First MeetingDarwin100% (1)
- Report On Health and Safety Organization Form (DOLE - BWC - OHSD - IP-5)Document2 paginiReport On Health and Safety Organization Form (DOLE - BWC - OHSD - IP-5)Randy Pedroza100% (6)
- Guide To Composition of Safety CommitteeDocument2 paginiGuide To Composition of Safety Committeeraighnejames1975% (4)
- MINUTES OF MEETING AprilDocument2 paginiMINUTES OF MEETING AprilAlvin John DionisioÎncă nu există evaluări
- Alcohol-Free Workplace Policy & ProgramDocument4 paginiAlcohol-Free Workplace Policy & Programraighnejames1950% (2)
- Mandatory 8-Hours Safety and Health SeminarDocument170 paginiMandatory 8-Hours Safety and Health SeminarSamuel Pobre86% (21)
- Dole No Pending CaseDocument2 paginiDole No Pending CaseJaycie Ponseca Ambito0% (1)
- Rso DoleDocument1 paginăRso DoleRERREFAIT100% (1)
- Memorandum TO: Cbti Employee, Security Guards, Contractor/Subcontractor From: Cbti-Hsse Date: JUNE 19, 2020 RE: Personal Protective EquipmentDocument1 paginăMemorandum TO: Cbti Employee, Security Guards, Contractor/Subcontractor From: Cbti-Hsse Date: JUNE 19, 2020 RE: Personal Protective EquipmentJerick Villones100% (2)
- Breastfeeding Policy: Main Office Clark CDO Cebu Ilo-Ilo Davao Palawan WebsiteDocument2 paginiBreastfeeding Policy: Main Office Clark CDO Cebu Ilo-Ilo Davao Palawan Websitemark_ortencio100% (2)
- Bukidnon State University: Buksu Casisang AnnexDocument2 paginiBukidnon State University: Buksu Casisang Annexjason a. un100% (2)
- Safety Practitioner Accreditation ChecklistDocument2 paginiSafety Practitioner Accreditation Checklistrasales100% (4)
- Hepatitis B Workplace Policy & ProgramDocument4 paginiHepatitis B Workplace Policy & Programraighnejames1950% (2)
- Description of Existing Solid Waste Management Plan - Aart Id NumberDocument1 paginăDescription of Existing Solid Waste Management Plan - Aart Id NumberDiane Bonilla Lacena50% (2)
- Minutes of The Meeting - DoleDocument1 paginăMinutes of The Meeting - DoleIvy Claris Ba-awa Iquin100% (1)
- Application Form For Permit To Operate (PTO) Air Pollution Source InstallationsDocument3 paginiApplication Form For Permit To Operate (PTO) Air Pollution Source InstallationsMiguel Antonio Uy EscolarÎncă nu există evaluări
- Cost of OSH BreakdownDocument1 paginăCost of OSH BreakdownPau ContrerasÎncă nu există evaluări
- EwairDocument1 paginăEwairAlaine SobredoÎncă nu există evaluări
- WAIRDocument1 paginăWAIRAlaine SobredoÎncă nu există evaluări
- Accreditation No.: 1030-091918-093Document4 paginiAccreditation No.: 1030-091918-093Leo Buquiran AcabalÎncă nu există evaluări
- EWAIRDocument1 paginăEWAIRKissy AndarzaÎncă nu există evaluări
- Employer's Work Accident ReportDocument1 paginăEmployer's Work Accident ReportAlex Elle0% (1)
- Hot WorkDocument1 paginăHot WorkChipÎncă nu există evaluări
- Employer'S Work Accident/Illness ReportDocument1 paginăEmployer'S Work Accident/Illness ReportReynaldo PesqueraÎncă nu există evaluări
- Dole BWC Ohsd Ip 6Document1 paginăDole BWC Ohsd Ip 6Wenceslao Ogahayon BaguioÎncă nu există evaluări
- 3) EwarDocument1 pagină3) EwarREN OFFICIALÎncă nu există evaluări
- Plea BargainingDocument3 paginiPlea BargainingМарк Артём Лимот АпаллаÎncă nu există evaluări
- Torts CasesDocument18 paginiTorts CasesМарк Артём Лимот АпаллаÎncă nu există evaluări
- Rules of Procedure For Environmental CasesDocument13 paginiRules of Procedure For Environmental CasesМарк Артём Лимот АпаллаÎncă nu există evaluări
- DNA EvidenceDocument8 paginiDNA EvidenceМарк Артём Лимот АпаллаÎncă nu există evaluări
- Plea BargainingDocument3 paginiPlea BargainingМарк Артём Лимот АпаллаÎncă nu există evaluări
- Jposta. Barbara LPG Plant Safety AuditDocument16 paginiJposta. Barbara LPG Plant Safety AuditМарк Артём Лимот Апалла80% (5)
- Report of Safety and Health OrganizationDocument1 paginăReport of Safety and Health OrganizationМарк Артём Лимот АпаллаÎncă nu există evaluări
- Report of Safety and Health Organization MarilaoDocument1 paginăReport of Safety and Health Organization MarilaoМарк Артём Лимот АпаллаÎncă nu există evaluări
- Toledo Accomplishment ReportDocument2 paginiToledo Accomplishment ReportМарк Артём Лимот АпаллаÎncă nu există evaluări
- Travel OrderDocument1 paginăTravel OrderМарк Артём Лимот АпаллаÎncă nu există evaluări
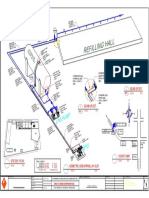
- Lighting Layout Power Layout: LPG Refilling PlantDocument1 paginăLighting Layout Power Layout: LPG Refilling PlantМарк Артём Лимот АпаллаÎncă nu există evaluări
- Annual Medical ReportDocument1 paginăAnnual Medical ReportМарк Артём Лимот АпаллаÎncă nu există evaluări
- Format For Fire Safety Equipment InventoryDocument3 paginiFormat For Fire Safety Equipment InventoryМарк Артём Лимот АпаллаÎncă nu există evaluări
- Plant LayoutDocument1 paginăPlant LayoutМарк Артём Лимот АпаллаÎncă nu există evaluări
- Schedule of Loads: LPG Refilling PlantDocument1 paginăSchedule of Loads: LPG Refilling PlantМарк Артём Лимот АпаллаÎncă nu există evaluări
- Prycegas LPG Personnel (Trainee)Document2 paginiPrycegas LPG Personnel (Trainee)Марк Артём Лимот АпаллаÎncă nu există evaluări
- PRYCEGAS LPG PERSONNEL (Supervisory)Document4 paginiPRYCEGAS LPG PERSONNEL (Supervisory)Марк Артём Лимот Апалла100% (2)
- Format 2018 Plant Equipment InventoryDocument4 paginiFormat 2018 Plant Equipment InventoryМарк Артём Лимот АпаллаÎncă nu există evaluări
- Summative Assessment Lesson PlanDocument4 paginiSummative Assessment Lesson Planapi-363015523Încă nu există evaluări
- Handbook GoodwillDocument73 paginiHandbook Goodwillkey2careersÎncă nu există evaluări
- Wqu Catalog 2019Document52 paginiWqu Catalog 2019Victor FrankensteinÎncă nu există evaluări
- 2 Maersk Filipinas V RamosDocument11 pagini2 Maersk Filipinas V RamosFrances Angelica Domini KoÎncă nu există evaluări
- Profile For Females: Conners' Parent Rating Scale-Revised (S)Document2 paginiProfile For Females: Conners' Parent Rating Scale-Revised (S)Claudya Abarca50% (8)
- 2020 2025 Fuwavita Strategic Plan 1Document25 pagini2020 2025 Fuwavita Strategic Plan 1María EugeniaÎncă nu există evaluări
- VIB Chapter-I PDFDocument6 paginiVIB Chapter-I PDFashurieÎncă nu există evaluări
- Response BlockingDocument3 paginiResponse Blockingiulia9gavris50% (2)
- Diversification and Inclusion: Pilipinas Shell Petroleum CorporationDocument17 paginiDiversification and Inclusion: Pilipinas Shell Petroleum CorporationBeatriz VillanuevaÎncă nu există evaluări
- Physical Therapy DocumentationDocument160 paginiPhysical Therapy Documentationdaniel arayaÎncă nu există evaluări
- 6 Disability Certification in PsychiatryDocument20 pagini6 Disability Certification in PsychiatryMegha JainÎncă nu există evaluări
- Module 1 Prof. Ed 4 1st Sem 2021-2022Document20 paginiModule 1 Prof. Ed 4 1st Sem 2021-2022Angelica PardeñoÎncă nu există evaluări
- Annual MSWD Accomplishment Report 2021Document13 paginiAnnual MSWD Accomplishment Report 2021MSWD BAMBANG100% (1)
- Medical SociologyDocument14 paginiMedical SociologymymagicookieÎncă nu există evaluări
- PREVIEW FORM - Australia Awards Scholarships Application Form PHD and Master Intake 2024 PDFDocument21 paginiPREVIEW FORM - Australia Awards Scholarships Application Form PHD and Master Intake 2024 PDFferi styaningsihÎncă nu există evaluări
- Effects of COVID-19 On Children's Mental HealthDocument21 paginiEffects of COVID-19 On Children's Mental Healthduwa douglasÎncă nu există evaluări
- 02 Dwornik CopyEdited 22 2 FinalDocument16 pagini02 Dwornik CopyEdited 22 2 FinalShir LeyÎncă nu există evaluări
- Role of Assistive Technology in Teaching-Learning Process of The Students With Visual Impairment: An Insight StudyDocument19 paginiRole of Assistive Technology in Teaching-Learning Process of The Students With Visual Impairment: An Insight StudyAnonymous CwJeBCAXpÎncă nu există evaluări
- PART TWO - Preferred Practice PatternsDocument272 paginiPART TWO - Preferred Practice PatternsCherrie Anne MiguelÎncă nu există evaluări
- Arga Naufal Hilmi Rafif - 21010116120078Document9 paginiArga Naufal Hilmi Rafif - 21010116120078Fadhil FahrenzaÎncă nu există evaluări
- US Department of Justice Civil Rights Division - Letter - Tal244Document8 paginiUS Department of Justice Civil Rights Division - Letter - Tal244legalmattersÎncă nu există evaluări
- Marshawn Love LawsuitDocument21 paginiMarshawn Love LawsuitAsbury Park Press100% (1)
- Vba 21 526ez AreDocument10 paginiVba 21 526ez Arejim912Încă nu există evaluări
- Individual & Group ExercisesDocument16 paginiIndividual & Group ExercisesLakshmi Pavani100% (11)
- Lesson 6Document28 paginiLesson 6jveruasaÎncă nu există evaluări
- 2013 Psychaitric Nursing Problem StatementsDocument13 pagini2013 Psychaitric Nursing Problem StatementsMAHESH KOUJALAGI100% (3)
- Manabik Pension Scheme 2018Document8 paginiManabik Pension Scheme 2018priyamdawnÎncă nu există evaluări
- Free Disability e Book PartDocument500 paginiFree Disability e Book PartTony KelbratÎncă nu există evaluări
- Application For Employment Form 2Document10 paginiApplication For Employment Form 2Amoakoah Akosua GloriaÎncă nu există evaluări
- Intoduction To InclusiveDocument36 paginiIntoduction To InclusivePrincess Fenix SabioÎncă nu există evaluări