S-ar putea să vă placă și
- Adolescent Reproductive and Sexual Health PromotioDocument13 paginiAdolescent Reproductive and Sexual Health PromotiolzbthdukerÎncă nu există evaluări
- Social Determinants of Unintended Pregnancy and Maternal CareDocument29 paginiSocial Determinants of Unintended Pregnancy and Maternal Carelestari pamungkas100% (1)
- Adolescent Demand For Contraception and Family Planning Services in Low-And Middle-Income Countries: A Systematic ReviewDocument20 paginiAdolescent Demand For Contraception and Family Planning Services in Low-And Middle-Income Countries: A Systematic ReviewMusie KurabachewÎncă nu există evaluări
- Fertility Awareness, Attitudes Towards Parenting, and Knowledge About Assisted Reproductive Technology Among University Students in ArgentinaDocument6 paginiFertility Awareness, Attitudes Towards Parenting, and Knowledge About Assisted Reproductive Technology Among University Students in ArgentinaAneley FerreyraÎncă nu există evaluări
- PM en AdolecentesDocument5 paginiPM en AdolecentescesarÎncă nu există evaluări
- Healthy Babies Are Worth The Wait: A Partnership to Reduce Preterm Births in Kentucky through Community-based Interventions 2007 - 2009De la EverandHealthy Babies Are Worth The Wait: A Partnership to Reduce Preterm Births in Kentucky through Community-based Interventions 2007 - 2009Încă nu există evaluări
- Meta 2Document14 paginiMeta 2S2-IKM ULMÎncă nu există evaluări
- Abortion Knowledge Attitudes and Experiences Among Adolescent Girls A Review of The LiteratureDocument22 paginiAbortion Knowledge Attitudes and Experiences Among Adolescent Girls A Review of The LiteratureFake_Me_Încă nu există evaluări
- Investigating Determinants Influencing Contraceptive Adoption Among Third-Year Medical Students A Study at KIU-WC Bushenyi District, Western UgandaDocument12 paginiInvestigating Determinants Influencing Contraceptive Adoption Among Third-Year Medical Students A Study at KIU-WC Bushenyi District, Western UgandaKIU PUBLICATION AND EXTENSIONÎncă nu există evaluări
- Estimating abortion incidence among adolescents and differences in postabortion care by ageDocument7 paginiEstimating abortion incidence among adolescents and differences in postabortion care by ageWalter MendozaÎncă nu există evaluări
- Research Paper AidsDocument4 paginiResearch Paper Aidsc9hpjcb3100% (1)
- The Level of Awareness of Argao National High School Students About Contraceptives and Teenage PregnancyDocument139 paginiThe Level of Awareness of Argao National High School Students About Contraceptives and Teenage Pregnancysanielmike123Încă nu există evaluări
- Journal of The International AIDS Society - 2019 - Martins - Prevalence and Factors Associated With Fertility DesiresDocument22 paginiJournal of The International AIDS Society - 2019 - Martins - Prevalence and Factors Associated With Fertility DesiresAndrade GuiÎncă nu există evaluări
- Interbirth Intervals of Immigrant and Refugee Women in The United States - A Cross-Sectional StudyDocument10 paginiInterbirth Intervals of Immigrant and Refugee Women in The United States - A Cross-Sectional StudyRENUKADEVIÎncă nu există evaluări
- The Nature and Extent of COVID 19 Vaccination Hesitancy in Healthcare WorkersDocument8 paginiThe Nature and Extent of COVID 19 Vaccination Hesitancy in Healthcare WorkersamiryahiaÎncă nu există evaluări
- Journal of The International AIDS Society - 2023 - Bernays - They Test My Blood To Know How Much Blood Is in My Body TheDocument9 paginiJournal of The International AIDS Society - 2023 - Bernays - They Test My Blood To Know How Much Blood Is in My Body TheFiraol MesfinÎncă nu există evaluări
- Dela Cruz & Dy - Media JournalDocument11 paginiDela Cruz & Dy - Media JournalZach Daniel Dela CruzÎncă nu există evaluări
- Annotated Source List - Ayaz 2Document9 paginiAnnotated Source List - Ayaz 2api-615502029Încă nu există evaluări
- Defining Misinformation and Related Terms in Health-Related Literature Scoping ReviewDocument11 paginiDefining Misinformation and Related Terms in Health-Related Literature Scoping Reviewmanuelserodio.argÎncă nu există evaluări
- From Science To Sustainable Systems: Evidence Based-Decision Making For Adolescent Fertility in ZambiaDocument6 paginiFrom Science To Sustainable Systems: Evidence Based-Decision Making For Adolescent Fertility in ZambiaMargarateÎncă nu există evaluări
- Vaginal Ring Acceptability and Related Preferences Among Women in Low-And Middle-Income Countries: A Systematic Review and Narrative SynthesisDocument22 paginiVaginal Ring Acceptability and Related Preferences Among Women in Low-And Middle-Income Countries: A Systematic Review and Narrative Synthesislidwina143Încă nu există evaluări
- Knowledge and Use of Contraceptives Improved by Health EducationDocument14 paginiKnowledge and Use of Contraceptives Improved by Health EducationArdin MunrekÎncă nu există evaluări
- Meta AnalisisDocument11 paginiMeta AnalisisS2-IKM ULMÎncă nu există evaluări
- IUFD Incidence Causes and Complications A RetrospeDocument6 paginiIUFD Incidence Causes and Complications A Retrospeadri20121989Încă nu există evaluări
- Global Strategy For Women's, Children's and Adolescents' Health (2016-2030)Document6 paginiGlobal Strategy For Women's, Children's and Adolescents' Health (2016-2030)Portal HDÎncă nu există evaluări
- Children 09 01511Document17 paginiChildren 09 01511Łukasz SzymańskiÎncă nu există evaluări
- 1472 6874 10 8 PDFDocument7 pagini1472 6874 10 8 PDFhirsi200518Încă nu există evaluări
- Promoting Fertility Awareness and Preconception Health Using A Chatbot: A Randomized Controlled TrialDocument11 paginiPromoting Fertility Awareness and Preconception Health Using A Chatbot: A Randomized Controlled TrialGetz23Încă nu există evaluări
- Understanding Vaccination Knowledge, Attitude, and Perception Among Women Regarding Immunization During Pregnancy in Riyadh, Saudi ArabiaDocument8 paginiUnderstanding Vaccination Knowledge, Attitude, and Perception Among Women Regarding Immunization During Pregnancy in Riyadh, Saudi ArabiaIJAR JOURNALÎncă nu există evaluări
- Literature Review On StillbirthDocument6 paginiLiterature Review On Stillbirthaflsvagfb100% (1)
- NakiDocument23 paginiNakiainamaniÎncă nu există evaluări
- Lilian FPDocument24 paginiLilian FPhenri kaneÎncă nu există evaluări
- 10 - Dwiti Hikmah Sari - 16ik466Document11 pagini10 - Dwiti Hikmah Sari - 16ik466titi hikmahsariÎncă nu există evaluări
- Association Between Media Exposure and Family Planning in Myanmar and Philippines: Evidence From Nationally Representative Survey DataDocument12 paginiAssociation Between Media Exposure and Family Planning in Myanmar and Philippines: Evidence From Nationally Representative Survey DataShiengCamachoÎncă nu există evaluări
- Art 2 EtsDocument17 paginiArt 2 EtsissisÎncă nu există evaluări
- Literature Review On Birth PreparednessDocument5 paginiLiterature Review On Birth Preparednessmgrekccnd100% (1)
- Attachment (64) 1Document15 paginiAttachment (64) 1lisavalentinsÎncă nu există evaluări
- Full Proposal - Factors Contributing To Abortions Among The Youths Between The Ages 15 and 30 Years Old at Chipata Central Hospital.Document24 paginiFull Proposal - Factors Contributing To Abortions Among The Youths Between The Ages 15 and 30 Years Old at Chipata Central Hospital.gomaÎncă nu există evaluări
- Knowledge, Attitude and Practice Related To Reproductive Health Among Female AdolescentsDocument13 paginiKnowledge, Attitude and Practice Related To Reproductive Health Among Female AdolescentsAbdullah SiddiqÎncă nu există evaluări
- Promising Practices For The Design and Implementation of Sexuality Education Programmes For Youth in India A Scoping ReviewDocument31 paginiPromising Practices For The Design and Implementation of Sexuality Education Programmes For Youth in India A Scoping ReviewRahul YaDaVÎncă nu există evaluări
- Factors Associated With Pregnancy Among Filipino Women Aged 15-19: Results From The 2017 Philippine National Demographic and Health SurveyDocument15 paginiFactors Associated With Pregnancy Among Filipino Women Aged 15-19: Results From The 2017 Philippine National Demographic and Health SurveyJames Vincent DiazÎncă nu există evaluări
- Ca MamaeDocument7 paginiCa MamaeAnonymous vkq7UwÎncă nu există evaluări
- CHAPTER ONE by MohamedDocument10 paginiCHAPTER ONE by Mohamedibrahimkulow999Încă nu există evaluări
- archivev3i3MDIwMTMxMjQ3 PDFDocument7 paginiarchivev3i3MDIwMTMxMjQ3 PDFLatasha WilderÎncă nu există evaluări
- Research Group 3 FinalDocument18 paginiResearch Group 3 FinalPhilip memezÎncă nu există evaluări
- Epidemiology Thesis PaperDocument4 paginiEpidemiology Thesis Paperlindsayalstonatlanta100% (2)
- Reproductive Health Indicators - Moving ForwardDocument36 paginiReproductive Health Indicators - Moving ForwardEden TesfayeÎncă nu există evaluări
- FulltextDocument19 paginiFulltextibrahimÎncă nu există evaluări
- Influence of Broadcast Media Campaigns On Creating Awareness On Exclusive Breastfeeding: A Study of Owerri UrbanDocument9 paginiInfluence of Broadcast Media Campaigns On Creating Awareness On Exclusive Breastfeeding: A Study of Owerri Urbanmonojoonk94Încă nu există evaluări
- Annotated BibliographyDocument12 paginiAnnotated BibliographyJOSEPHÎncă nu există evaluări
- Setting research priorities to improve access to family planningDocument12 paginiSetting research priorities to improve access to family planningtining sulistyowatiÎncă nu există evaluări
- Literature Review On Neonatal DeathDocument6 paginiLiterature Review On Neonatal Deathafdtovmhb100% (1)
- Application of Data Mining Techniques To Predict Adult Mortality Thecase of Butajira Rural Health Program Butajira Ethiopia 2157 7420 1000197Document10 paginiApplication of Data Mining Techniques To Predict Adult Mortality Thecase of Butajira Rural Health Program Butajira Ethiopia 2157 7420 1000197Anonymous siuYVkSmdÎncă nu există evaluări
- Understanding the Complex Factors Driving Vaccine Hesitancy in 40 CharactersDocument6 paginiUnderstanding the Complex Factors Driving Vaccine Hesitancy in 40 CharactersAlexandra Mae D. MiguelÎncă nu există evaluări
- Awareness About Reproductive Health Issues Among Adolescents - A ReviewDocument3 paginiAwareness About Reproductive Health Issues Among Adolescents - A ReviewInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Journal Health CareDocument10 paginiJournal Health CareMeidita Annisa PurmanÎncă nu există evaluări
- Health Information On The Internet: The Case of GreeceDocument12 paginiHealth Information On The Internet: The Case of GreecemaryÎncă nu există evaluări
- Research Paper Topics About HivDocument8 paginiResearch Paper Topics About Hivlrqylwznd100% (1)
- SRHR2 - EWEC Advocacy Roadmap 2017 - FinalDocument3 paginiSRHR2 - EWEC Advocacy Roadmap 2017 - FinalManoj MaharjanÎncă nu există evaluări
- Social Determinants of Health and Knowledge About Hiv/Aids Transmission Among AdolescentsDe la EverandSocial Determinants of Health and Knowledge About Hiv/Aids Transmission Among AdolescentsÎncă nu există evaluări
- Lynch Et Al-2017-Cochrane Database of Systematic ReviewsDocument13 paginiLynch Et Al-2017-Cochrane Database of Systematic Reviewsrais123Încă nu există evaluări
- Strength Training Protocols in Hemiparetic Individuals Post Stroke: A Systematic ReviewDocument11 paginiStrength Training Protocols in Hemiparetic Individuals Post Stroke: A Systematic Reviewrais123Încă nu există evaluări
- Very Early Versus Delayed Mobilisation After Stroke (Protocol)Document8 paginiVery Early Versus Delayed Mobilisation After Stroke (Protocol)rais123Încă nu există evaluări
- Cortical Thickness in Obsessive-Compulsive Disorder: Multisite Mega-Analysis of 780 Brain Scans From Six CentresDocument19 paginiCortical Thickness in Obsessive-Compulsive Disorder: Multisite Mega-Analysis of 780 Brain Scans From Six Centresrais123Încă nu există evaluări
- Very Early Versus Delayed Mobilisation After Stroke (Protocol)Document8 paginiVery Early Versus Delayed Mobilisation After Stroke (Protocol)rais123Încă nu există evaluări
- Sexual Orientation and Suicidal Behaviour in Adolescents and Young Adults: Systematic Review and Meta-AnalysisDocument25 paginiSexual Orientation and Suicidal Behaviour in Adolescents and Young Adults: Systematic Review and Meta-Analysisrais123Încă nu există evaluări
- Very Early Versus Delayed Mobilisation After Stroke (Protocol)Document8 paginiVery Early Versus Delayed Mobilisation After Stroke (Protocol)rais123Încă nu există evaluări
- ASC Rehabilitation Literature Review Final Report December 20101 PDFDocument14 paginiASC Rehabilitation Literature Review Final Report December 20101 PDFrais123Încă nu există evaluări
- Outcomes of Return-To-Work After Stroke Rehabilitation: A Systematic ReviewDocument11 paginiOutcomes of Return-To-Work After Stroke Rehabilitation: A Systematic Reviewrais123Încă nu există evaluări
- Very Early Versus Delayed Mobilisation After Stroke (Protocol)Document8 paginiVery Early Versus Delayed Mobilisation After Stroke (Protocol)rais123Încă nu există evaluări
- Iwan Jurnal77Document7 paginiIwan Jurnal77IwanÎncă nu există evaluări
- Faktor Yang Memengaruhi Pemilihan Metode KontrasepsiDocument8 paginiFaktor Yang Memengaruhi Pemilihan Metode Kontrasepsirais123Încă nu există evaluări
- 5Document8 pagini5Nining Rhyanie TampubolonÎncă nu există evaluări
- OpthalmologiDocument7 paginiOpthalmologirais123Încă nu există evaluări
- Ocular Allergy: An Updated Review: January 2017Document8 paginiOcular Allergy: An Updated Review: January 2017rais123Încă nu există evaluări
- Traumatic Cataract Jurnal of Ocular BiologyDocument4 paginiTraumatic Cataract Jurnal of Ocular BiologyajimÎncă nu există evaluări
- Neuroimmunology: Clinical Characteristics of Autoimmune Optic NeuritisDocument9 paginiNeuroimmunology: Clinical Characteristics of Autoimmune Optic Neuritisrais123Încă nu există evaluări
- Steroid-induced Glaucoma: An Avoidable BlindnessDocument6 paginiSteroid-induced Glaucoma: An Avoidable Blindnessrais123Încă nu există evaluări
- 413729Document5 pagini413729Rima WulansariÎncă nu există evaluări
- Personality and Uveitis PDFDocument6 paginiPersonality and Uveitis PDFrais123Încă nu există evaluări
- L1 Elements, Processed Pseudogene in MammalianDocument9 paginiL1 Elements, Processed Pseudogene in Mammalianrais123Încă nu există evaluări
- Ocular Allergy: An Updated Review: January 2017Document8 paginiOcular Allergy: An Updated Review: January 2017rais123Încă nu există evaluări
- Pseudo GenesDocument4 paginiPseudo Genesrais123Încă nu există evaluări
- Jurnal FixDocument9 paginiJurnal Fixrais123Încă nu există evaluări
- Data in Brief Volume 13 Issue 2017 -Doi 10.1016-2Fj.dib.2017.05.024- Gunbin, Konstantin_ Peshkin, Leonid_ Popadin, Konstantin_ Annis, -- Data on the Time of Integration of the Human Mitochondrial PseuDocument8 paginiData in Brief Volume 13 Issue 2017 -Doi 10.1016-2Fj.dib.2017.05.024- Gunbin, Konstantin_ Peshkin, Leonid_ Popadin, Konstantin_ Annis, -- Data on the Time of Integration of the Human Mitochondrial Pseurais123Încă nu există evaluări
- Pi Is 1063458416302928Document7 paginiPi Is 1063458416302928rais123Încă nu există evaluări
- Transposase PseudogeneDocument8 paginiTransposase Pseudogenerais123Încă nu există evaluări
- Bedside Diagnostics in Dermatology: Parasitic and Noninfectious DiseasesDocument10 paginiBedside Diagnostics in Dermatology: Parasitic and Noninfectious Diseasesrais123Încă nu există evaluări
- Comparison of Culture and PCR Methods in The Diagnosis of Bacterial MeningitisDocument5 paginiComparison of Culture and PCR Methods in The Diagnosis of Bacterial Meningitisrais123Încă nu există evaluări
- Science & Justice: Nina SundeDocument11 paginiScience & Justice: Nina SundeZulfia Retnanti MarissaÎncă nu există evaluări
- Mathematical Reliability TheoryDocument7 paginiMathematical Reliability Theoryjto777100% (1)
- Attachment insecurity and breadcrumbing - cross cultural between india and spainDocument11 paginiAttachment insecurity and breadcrumbing - cross cultural between india and spainAkanksha MehtaÎncă nu există evaluări
- Managing MNC Expatriates Through Crises: A Challenge For International Human Resource ManagementDocument3 paginiManaging MNC Expatriates Through Crises: A Challenge For International Human Resource Managementswapnil palÎncă nu există evaluări
- Cyber Strategy - The Evolving Character of Power and Coercion (Review)Document5 paginiCyber Strategy - The Evolving Character of Power and Coercion (Review)Luiza FonsecaÎncă nu există evaluări
- Quantitative Aptitude - Simplification - Free Aptitude PracticeDocument9 paginiQuantitative Aptitude - Simplification - Free Aptitude PracticeRaJu SinGhÎncă nu există evaluări
- Epi FinalDocument481 paginiEpi FinalSana Savana Aman R100% (1)
- Environment, Health & Safety: Operate in TheDocument12 paginiEnvironment, Health & Safety: Operate in TheCokongÎncă nu există evaluări
- Tools For Performance PDFDocument16 paginiTools For Performance PDFtalaboseÎncă nu există evaluări
- Ual Project Proposal Year 1 Final ProductDocument7 paginiUal Project Proposal Year 1 Final Productapi-531565793Încă nu există evaluări
- Reflection About Threats To Biodiversity and Thought Piece About Extreme MeasuresDocument2 paginiReflection About Threats To Biodiversity and Thought Piece About Extreme MeasuresNiña Dae GambanÎncă nu există evaluări
- BMGT Industries selects robotic projectsDocument3 paginiBMGT Industries selects robotic projectsJean Marcos Cueva SanchezÎncă nu există evaluări
- Evaluating The Igraph Community Detection AlgorithmsDocument8 paginiEvaluating The Igraph Community Detection AlgorithmsAmit BholaÎncă nu există evaluări
- Value of InformationDocument8 paginiValue of InformationKhushboo Arora100% (1)
- VVV V: V V VVV VVV V VV VVV VV VDocument11 paginiVVV V: V V VVV VVV V VV VVV VV Vnishasadanandam8637Încă nu există evaluări
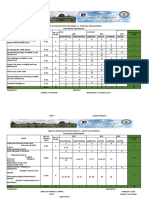
- Table of Specification For Grade 12 - Personal Development First Quarter ExaminationDocument17 paginiTable of Specification For Grade 12 - Personal Development First Quarter ExaminationArgie Joy Marie AmpolÎncă nu există evaluări
- LS-Dyna Simulated Crack in Several WaysDocument2 paginiLS-Dyna Simulated Crack in Several WaysMubeenÎncă nu există evaluări
- Entrepreneurship Lecture Number 5 6 and 7Document36 paginiEntrepreneurship Lecture Number 5 6 and 7UMAIR TARIQ L1F17BBAM0054Încă nu există evaluări
- Vinit Kumar Gunjan, Vicente Garcia Diaz, Manuel Cardona, Vijender Kumar Solanki, K. V. N. Sunitha - ICICCT 2019 – System Reliability, Quality Control, Safety, Maintenance and Management_ Applications .pdfDocument894 paginiVinit Kumar Gunjan, Vicente Garcia Diaz, Manuel Cardona, Vijender Kumar Solanki, K. V. N. Sunitha - ICICCT 2019 – System Reliability, Quality Control, Safety, Maintenance and Management_ Applications .pdfepieÎncă nu există evaluări
- Optimization of Machining Parameters On AL 6061 Alloy Using Response Surface MethodologyDocument5 paginiOptimization of Machining Parameters On AL 6061 Alloy Using Response Surface MethodologySotu KdaptÎncă nu există evaluări
- EFQM Business Excellence ModelDocument5 paginiEFQM Business Excellence Modelmarrisha26Încă nu există evaluări
- How To Analyse Questionnaire ResponsesDocument2 paginiHow To Analyse Questionnaire ResponsesRolly JameroÎncă nu există evaluări
- Unexplored Gamification Elements in Learning Environments: Sara Adel El-Shorbagy, Nada Sherief, Walid AbdelmoezDocument6 paginiUnexplored Gamification Elements in Learning Environments: Sara Adel El-Shorbagy, Nada Sherief, Walid AbdelmoezSneha MajiÎncă nu există evaluări
- A Brief Guide To Structural Equation ModelingDocument33 paginiA Brief Guide To Structural Equation Modelingprakash_kediaÎncă nu există evaluări
- Cyient - Oil and Gas IndustryDocument8 paginiCyient - Oil and Gas Industrycyient_analyticsÎncă nu există evaluări
- ANALYZE - The Influence of Social MediaDocument4 paginiANALYZE - The Influence of Social MediaSvAnimeÎncă nu există evaluări
- Information Retrieval Course Outline Nov 2014 FSTS 1Document2 paginiInformation Retrieval Course Outline Nov 2014 FSTS 1Mubaarak NuurÎncă nu există evaluări
- End of Chapter QuestionsDocument4 paginiEnd of Chapter QuestionsFritz NatividadÎncă nu există evaluări
- Title of Project: Box 16. GAD Checklist For Project Management and ImplementationDocument7 paginiTitle of Project: Box 16. GAD Checklist For Project Management and ImplementationArniel Fred Tormis FernandezÎncă nu există evaluări
- Term Paper Proposal - 20CH003Document6 paginiTerm Paper Proposal - 20CH003Abdulla Mamun100% (1)