S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Sample Employee Handbook Hr360Document39 paginiSample Employee Handbook Hr360Andi YanuarÎncă nu există evaluări
- Competency Matrix Form Sheet Rev 0Document3 paginiCompetency Matrix Form Sheet Rev 0Andi YanuarÎncă nu există evaluări
- Service Agreement TemplateDocument2 paginiService Agreement TemplateMathur DineshÎncă nu există evaluări
- VCSU Staff Performance & Compensation ModelDocument16 paginiVCSU Staff Performance & Compensation ModelAndi YanuarÎncă nu există evaluări
- Service Level Agreement: (Company Name)Document21 paginiService Level Agreement: (Company Name)Radhika SÎncă nu există evaluări
- Levinson - CompensationDocument30 paginiLevinson - CompensationAndi YanuarÎncă nu există evaluări
- Sample Job Offer LetterDocument1 paginăSample Job Offer LetterAndi YanuarÎncă nu există evaluări
- KPI Table for Business PerformanceDocument24 paginiKPI Table for Business PerformanceJonathan Morales100% (9)
- Format - Appraisal FormDocument6 paginiFormat - Appraisal FormAndi YanuarÎncă nu există evaluări
- Employment BenefitsDocument44 paginiEmployment BenefitsSharmila BalasubramaniÎncă nu există evaluări
- Employment BenefitsDocument44 paginiEmployment BenefitsSharmila BalasubramaniÎncă nu există evaluări
- Chart PPT Template 024Document2 paginiChart PPT Template 024Andi YanuarÎncă nu există evaluări
- Perjanjian Kerja Untuk Waktu Tertentu (Perjanjian Kerja Kontrak) Perlu DitertibkanDocument15 paginiPerjanjian Kerja Untuk Waktu Tertentu (Perjanjian Kerja Kontrak) Perlu DitertibkanAndi YanuarÎncă nu există evaluări
- VCSU Staff Performance & Compensation ModelDocument16 paginiVCSU Staff Performance & Compensation ModelAndi YanuarÎncă nu există evaluări
- VP Product Development JobDocument2 paginiVP Product Development JobAndi YanuarÎncă nu există evaluări
- Job Description - Bussiness Development ExecutiveDocument2 paginiJob Description - Bussiness Development ExecutiveAndi YanuarÎncă nu există evaluări
- VP Product Development JobDocument2 paginiVP Product Development JobAndi YanuarÎncă nu există evaluări
- Teori Harga PasarDocument53 paginiTeori Harga PasarAndi YanuarÎncă nu există evaluări
- Indonesia 2017 Salary GuideDocument48 paginiIndonesia 2017 Salary Guidediki100% (2)
- Training EvaluationDocument49 paginiTraining EvaluationMuhammad Saqib AsifÎncă nu există evaluări
- Kpi Development For Hse PDFDocument229 paginiKpi Development For Hse PDFJunard M. Lu Hap100% (3)
- 006 E019Document5 pagini006 E019Andi YanuarÎncă nu există evaluări
- Allpipe Skills MatrixDocument58 paginiAllpipe Skills MatrixAndi YanuarÎncă nu există evaluări
- AkzoNobel KPIs Overview tcm9-38549 PDFDocument1 paginăAkzoNobel KPIs Overview tcm9-38549 PDFAndi YanuarÎncă nu există evaluări
- Allpipe Skills MatrixDocument58 paginiAllpipe Skills MatrixAndi YanuarÎncă nu există evaluări
- Membership InternDocument2 paginiMembership InternAndi YanuarÎncă nu există evaluări
- AkzoNobel KPIs Overview Tcm9-38549Document1 paginăAkzoNobel KPIs Overview Tcm9-38549Andi YanuarÎncă nu există evaluări
- Salaryguide2016indonesia 160420040251 PDFDocument10 paginiSalaryguide2016indonesia 160420040251 PDFAndi YanuarÎncă nu există evaluări
- HR Monthly Report (Contoh Formatlaporan Bulanan HR) : Oleh: Anwar SantosoDocument12 paginiHR Monthly Report (Contoh Formatlaporan Bulanan HR) : Oleh: Anwar SantosoAndi YanuarÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- FIN AL: Form GSTR-1Document5 paginiFIN AL: Form GSTR-1Pruthiv RajÎncă nu există evaluări
- Residency Final / On Account WHT Tax Code Rate %Document3 paginiResidency Final / On Account WHT Tax Code Rate %wilberforceÎncă nu există evaluări
- Chapter I: Introduction of Study: Goods and Service Tax (GST)Document73 paginiChapter I: Introduction of Study: Goods and Service Tax (GST)Prajakta KambleÎncă nu există evaluări
- BIR RULING (DA-380-03) : International Manning Agents, IncDocument6 paginiBIR RULING (DA-380-03) : International Manning Agents, IncHADTUGIÎncă nu există evaluări
- BIR Form 0605Document2 paginiBIR Form 0605Kathleen Anne CabreraÎncă nu există evaluări
- Assessment Form - TAXN6045 2020.2Document8 paginiAssessment Form - TAXN6045 2020.2bagasÎncă nu există evaluări
- Payslip PDFDocument1 paginăPayslip PDFNamasteÎncă nu există evaluări
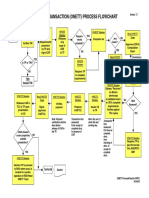
- One-Time Transaction (Onett) Process Flowchart: StartDocument1 paginăOne-Time Transaction (Onett) Process Flowchart: StartJenely Joy Areola-TelanÎncă nu există evaluări
- P3771 Payslip Dec2019 PDFDocument1 paginăP3771 Payslip Dec2019 PDFStalin Naveen KumarÎncă nu există evaluări
- Estate TaxDocument2 paginiEstate Taxucc second yearÎncă nu există evaluări
- TaxationDocument3 paginiTaxationMegumi HideyukiÎncă nu există evaluări
- Report of The BBI Steering CommitteeDocument204 paginiReport of The BBI Steering CommitteeThe Star Kenya100% (31)
- Training Design PPFIDocument7 paginiTraining Design PPFIJoy Peneyra DenostaÎncă nu există evaluări
- Indirect Taxes: Income TaxDocument9 paginiIndirect Taxes: Income TaxDanial ShadÎncă nu există evaluări
- Tax Returns Description Monthly Quarterly Annual Remarks: Companies Covered: Holding CompaniesDocument2 paginiTax Returns Description Monthly Quarterly Annual Remarks: Companies Covered: Holding CompaniesArvin GarciaÎncă nu există evaluări
- CDocument1 paginăCAakash GuptaÎncă nu există evaluări
- ContentsDocument5 paginiContentsshipraÎncă nu există evaluări
- Bir Form 0605Document4 paginiBir Form 0605Manoy BermeoÎncă nu există evaluări
- 3229 To 3233 Dollar Industries LimitedDocument2 pagini3229 To 3233 Dollar Industries LimitedmanjujeejooÎncă nu există evaluări
- TRAIN LAW TAX CALCULATORDocument5 paginiTRAIN LAW TAX CALCULATORKerwin Lester MandacÎncă nu există evaluări
- RA 7496-Simplified Net Income Scheme For Self-Employed & Professionals...Document5 paginiRA 7496-Simplified Net Income Scheme For Self-Employed & Professionals...Crislene CruzÎncă nu există evaluări
- Premium Certificate Financial Year 2020-2021 To Whomsoever It May ConcernDocument2 paginiPremium Certificate Financial Year 2020-2021 To Whomsoever It May ConcernmadhuÎncă nu există evaluări
- Topics On Income TaxationDocument4 paginiTopics On Income TaxationJessa Lopez GarciaÎncă nu există evaluări
- Direct Tax Vs Indirect TaxDocument22 paginiDirect Tax Vs Indirect TaxDr. Swati Gupta100% (1)
- Apartment Type Type A Type B Type C (4BHK+S.R) (3BHK+S.R) (3BHK) 3200 SQ FT 2350 SQ FT 1850 SQ FTDocument1 paginăApartment Type Type A Type B Type C (4BHK+S.R) (3BHK+S.R) (3BHK) 3200 SQ FT 2350 SQ FT 1850 SQ FTRohit ChhabraÎncă nu există evaluări
- GNV Tax News October 2021Document5 paginiGNV Tax News October 2021apriliaÎncă nu există evaluări
- Form 941 SummaryDocument5 paginiForm 941 SummaryCatori-Dakoda Eil100% (1)
- Earnings Statement: Non-NegotiableDocument1 paginăEarnings Statement: Non-NegotiableAyanna Sellers100% (5)
- SET 23 24 Detail Guide EDocument20 paginiSET 23 24 Detail Guide ENishan MahanamaÎncă nu există evaluări
- Chapter 11 Multiple Choice 2Document3 paginiChapter 11 Multiple Choice 2Mary DenizeÎncă nu există evaluări