S-ar putea să vă placă și
- ECMO Protocol AustraliaDocument17 paginiECMO Protocol AustraliaBiswarup Purkayastha100% (1)
- SKILL 8-16 Drawing Blood From A Central Venous Catheter: Key TermsDocument7 paginiSKILL 8-16 Drawing Blood From A Central Venous Catheter: Key TermsElizalde HusbandÎncă nu există evaluări
- Management of The EVDDocument7 paginiManagement of The EVDplethoraldork100% (1)
- Notes - Day 3 - MLB Class - FONDocument56 paginiNotes - Day 3 - MLB Class - FONVarsha ChudasmaÎncă nu există evaluări
- A Institutional Guideline-Procedure The Management of An IABP From The University of Maryland. Uploaded 2015Document3 paginiA Institutional Guideline-Procedure The Management of An IABP From The University of Maryland. Uploaded 2015alexÎncă nu există evaluări
- Acute ICU PT HandbookDocument52 paginiAcute ICU PT HandbookksdjlfkÎncă nu există evaluări
- CVP - Nursing Performance ChecklistDocument3 paginiCVP - Nursing Performance ChecklistJoy Jarin75% (4)
- Procedure-IABP InsertionDocument19 paginiProcedure-IABP Insertionmohamad dildarÎncă nu există evaluări
- Arterial Puncture InfosDocument9 paginiArterial Puncture InfosRuri DSÎncă nu există evaluări
- CH 2 SuctioningDocument90 paginiCH 2 SuctioningMaherÎncă nu există evaluări
- Insertion and Operation of IABP-1Document10 paginiInsertion and Operation of IABP-1Atia KiranÎncă nu există evaluări
- Suction Endotracheal V P StgeorgeDocument3 paginiSuction Endotracheal V P StgeorgeElaine Iris AbastaÎncă nu există evaluări
- I. Purpose: Clinical Practice Policy: Effective DateDocument7 paginiI. Purpose: Clinical Practice Policy: Effective DatesalamredÎncă nu există evaluări
- Central Lines AND Arterial LinesDocument41 paginiCentral Lines AND Arterial LinesSalinKaurÎncă nu există evaluări
- N.C.M. 106 Preliminary Exams Reviewer: Nyjil Patrick B. ColumbresDocument11 paginiN.C.M. 106 Preliminary Exams Reviewer: Nyjil Patrick B. ColumbresNyjil Patrick Basilio ColumbresÎncă nu există evaluări
- Final 16-17Document5 paginiFinal 16-17Churrizo IslamiÎncă nu există evaluări
- SP30 Neonatal Umbilical Vessel Catherization (Neonatal)Document13 paginiSP30 Neonatal Umbilical Vessel Catherization (Neonatal)Ritzjerald Christer Abrena PahilanÎncă nu există evaluări
- CVPDocument23 paginiCVPShalini KaluraÎncă nu există evaluări
- Whole Blood CollectionDocument16 paginiWhole Blood CollectionShemiza BalmacoonÎncă nu există evaluări
- BAL ProsedurDocument2 paginiBAL ProsedurisnanrÎncă nu există evaluări
- Specimen Collection Lab Safety BDocument55 paginiSpecimen Collection Lab Safety Bakoeljames8543Încă nu există evaluări
- Measurement of CENTRAL VENOUS PRESSURE Via A TransducerDocument22 paginiMeasurement of CENTRAL VENOUS PRESSURE Via A TransducerJasleen KaurÎncă nu există evaluări
- Arterial Lines MonitoringDocument13 paginiArterial Lines MonitoringJoseph Beredo33% (3)
- CVP MonitoringDocument10 paginiCVP MonitoringRaghu RajanÎncă nu există evaluări
- Specimen Collection and Transporation Instructions-1Document6 paginiSpecimen Collection and Transporation Instructions-1Marvel VisionÎncă nu există evaluări
- Central Venous CathetersDocument12 paginiCentral Venous CathetersarisastraÎncă nu există evaluări
- CHAPTER 10 SPECIAL PHLEBOTOMY AutosavedDocument104 paginiCHAPTER 10 SPECIAL PHLEBOTOMY AutosavedNorlyn Mae BihayÎncă nu există evaluări
- IV Therapy Learning Module Revised Sept21Document13 paginiIV Therapy Learning Module Revised Sept21Regean MercadoÎncă nu există evaluări
- HemodialysisDocument2 paginiHemodialysisJanelle MarceraÎncă nu există evaluări
- Nursing Care of Clients On Mechanical Ventilator For BSN IV StudentsDocument52 paginiNursing Care of Clients On Mechanical Ventilator For BSN IV Studentsspanishthingz01Încă nu există evaluări
- 11BBK Lec11 - Phlebotomy and Processing of Blood Sample MQA 2019-09-26 08-14-36Document24 pagini11BBK Lec11 - Phlebotomy and Processing of Blood Sample MQA 2019-09-26 08-14-36gothai sivapragasamÎncă nu există evaluări
- Pulmonary Artery Catheterization and MonitoringDocument31 paginiPulmonary Artery Catheterization and MonitoringVhince Norben PiscoÎncă nu există evaluări
- IV TherapyDocument39 paginiIV TherapyChannelGÎncă nu există evaluări
- Central Venous Catheters: Iv Terapy &Document71 paginiCentral Venous Catheters: Iv Terapy &Florence Liem0% (1)
- Acute/Critically Ill Patients in Hemodynamic Monitoring (Management)Document8 paginiAcute/Critically Ill Patients in Hemodynamic Monitoring (Management)Esmareldah Henry SirueÎncă nu există evaluări
- Technology Rules The World .Document71 paginiTechnology Rules The World .Lusy Octavia SaputriÎncă nu există evaluări
- Procedure For Patent Ductus Arteriosus (PDA) Device ClosureDocument13 paginiProcedure For Patent Ductus Arteriosus (PDA) Device ClosurejaganjaggiÎncă nu există evaluări
- IABP Slide Show Editor Zaychung - Pro.ksaDocument56 paginiIABP Slide Show Editor Zaychung - Pro.ksaZayChungÎncă nu există evaluări
- Groshong PICC and Catheters: Instructions For UseDocument20 paginiGroshong PICC and Catheters: Instructions For UseLucas FerreiraÎncă nu există evaluări
- 9 - ACLS - Part 1Document50 pagini9 - ACLS - Part 1Mohnmad ZaitoonÎncă nu există evaluări
- Peri - Operative ManagementDocument32 paginiPeri - Operative Managementrichamalik99Încă nu există evaluări
- Tugas Kelompok 2 BHS Inggris SopDocument17 paginiTugas Kelompok 2 BHS Inggris Sopmoms naraÎncă nu există evaluări
- The TandemheartDocument6 paginiThe TandemheartbencleeseÎncă nu există evaluări
- IV Therapy SsDocument56 paginiIV Therapy Sssaeed_chohan100% (8)
- One Lung Ventilation: Llalando L. Austin Ii, MHSC, Aa-C, RRT Nova Southeastern UniversityDocument47 paginiOne Lung Ventilation: Llalando L. Austin Ii, MHSC, Aa-C, RRT Nova Southeastern UniversityZulkarnainBustamam100% (1)
- SOP: Retro-Orbital Blood Collection in The RatDocument5 paginiSOP: Retro-Orbital Blood Collection in The RatSipend AnatomiÎncă nu există evaluări
- Central Venous Pressure Monitoring ManualDocument6 paginiCentral Venous Pressure Monitoring ManualCristina L. JaysonÎncă nu există evaluări
- Assisting IV BTDocument89 paginiAssisting IV BTmhelshy villanuevaÎncă nu există evaluări
- Ecmo PDFDocument5 paginiEcmo PDFAarti Dalwani100% (1)
- Abdominal AortaDocument41 paginiAbdominal AortaMichael IdowuÎncă nu există evaluări
- On IV TherapyDocument40 paginiOn IV TherapyDeology Juanino77% (13)
- Iv Cannulation: Dr. Carla O. Pandrya, Span FK UphDocument21 paginiIv Cannulation: Dr. Carla O. Pandrya, Span FK UphCandice LavigneÎncă nu există evaluări
- Tracheal Tubes and Prevention of VAPDocument23 paginiTracheal Tubes and Prevention of VAPعزالدين الزوقريÎncă nu există evaluări
- Master IV Answer WorksheetDocument4 paginiMaster IV Answer Worksheetworleyb83Încă nu există evaluări
- ABGS ProcedureDocument6 paginiABGS ProcedureHusson Ghalya100% (1)
- CVP PPPDocument13 paginiCVP PPPYep Yep100% (1)
- Venipuncture YmcDocument7 paginiVenipuncture Ymcdondon nobleÎncă nu există evaluări
- Anesthesiastudents 180625072546Document75 paginiAnesthesiastudents 180625072546Sashivaraman RajanÎncă nu există evaluări
- Survival Analysis, Part 3: Cox Regression: Statistics and Research DesignDocument2 paginiSurvival Analysis, Part 3: Cox Regression: Statistics and Research DesignGloria KartikaÎncă nu există evaluări
- MC GowanDocument13 paginiMC GowanGloria KartikaÎncă nu există evaluări
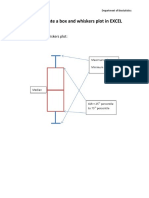
- How To Create A Box and Whiskers Plot in EXCELDocument9 paginiHow To Create A Box and Whiskers Plot in EXCELGloria KartikaÎncă nu există evaluări
- 24 Newsletter Hypertension and ArrhythmiaDocument2 pagini24 Newsletter Hypertension and ArrhythmiaGloria KartikaÎncă nu există evaluări
- CLN 66 01 107 PDFDocument5 paginiCLN 66 01 107 PDFGloria KartikaÎncă nu există evaluări
- Infeksi Marginalis NadaDocument48 paginiInfeksi Marginalis NadaGloria KartikaÎncă nu există evaluări
- Staining and Tooth DiscolorationDocument14 paginiStaining and Tooth DiscolorationGloria KartikaÎncă nu există evaluări
- Hypertension: H.) or May Be Associated With Other Diseases - Dorland'sDocument1 paginăHypertension: H.) or May Be Associated With Other Diseases - Dorland'sGloria KartikaÎncă nu există evaluări
- Righeimer ComplaintDocument45 paginiRigheimer ComplaintSarah BatchaÎncă nu există evaluări
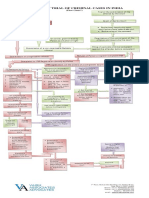
- Process of Trial of Criminal Cases in India (Flow Chart)Document1 paginăProcess of Trial of Criminal Cases in India (Flow Chart)Arun Hiro100% (1)
- FINAL Parent Handbook AitchisonDocument68 paginiFINAL Parent Handbook AitchisonSaeed AhmedÎncă nu există evaluări
- D245S 734046 Om enDocument90 paginiD245S 734046 Om enEndro Accoustic100% (1)
- The Value Relevance of Financial Statements and Their Impact On Stock PricesDocument18 paginiThe Value Relevance of Financial Statements and Their Impact On Stock Pricesanubha srivastavaÎncă nu există evaluări
- At The End of The Lesson, The Students Will Be Able To Apply The Indefinite Articles in The Given SentencesDocument11 paginiAt The End of The Lesson, The Students Will Be Able To Apply The Indefinite Articles in The Given SentencesRhielle Dimaculangan CabañezÎncă nu există evaluări
- Rock Classification Gizmo WorksheetDocument4 paginiRock Classification Gizmo WorksheetDiamond실비Încă nu există evaluări
- HTTP WWW - Aphref.aph - Gov.au House Committee Haa Overseasdoctors Subs Sub133Document3 paginiHTTP WWW - Aphref.aph - Gov.au House Committee Haa Overseasdoctors Subs Sub133hadia duraniÎncă nu există evaluări
- 5fcef6e7-HSM 2015 Student Edition IN3 V2Document788 pagini5fcef6e7-HSM 2015 Student Edition IN3 V2Ashvath Srinivas100% (2)
- 39 Storey Treehouse Activity Pack PDFDocument11 pagini39 Storey Treehouse Activity Pack PDFNeptune Shell0% (3)
- Bibliografia Antenas y RadioDocument3 paginiBibliografia Antenas y RadioJorge HerreraÎncă nu există evaluări
- Divorce: in The PhilippinesDocument4 paginiDivorce: in The PhilippinesKidMonkey2299Încă nu există evaluări
- đề thi TADocument15 paginiđề thi TAĐào Nguyễn Duy TùngÎncă nu există evaluări
- Edu602 Ubd TemplateDocument2 paginiEdu602 Ubd Templateapi-481192424Încă nu există evaluări
- Jamaica Sloane Conference Brochure-1Document4 paginiJamaica Sloane Conference Brochure-1labrishÎncă nu există evaluări
- PolygonsDocument23 paginiPolygonsPietrelle Liana PuruggananÎncă nu există evaluări
- Influence of Brand Experience On CustomerDocument16 paginiInfluence of Brand Experience On Customerarif adrianÎncă nu există evaluări
- Test A 10 - 12520231610Document2 paginiTest A 10 - 12520231610Quang HuyÎncă nu există evaluări
- Surimi Technology: Submitted To: Dr.A.K.Singh (Sr. Scientist) Submitted By: Rahul Kumar (M.Tech, DT, 1 Year)Document13 paginiSurimi Technology: Submitted To: Dr.A.K.Singh (Sr. Scientist) Submitted By: Rahul Kumar (M.Tech, DT, 1 Year)rahuldtc100% (2)
- Fin - e - 178 - 2022-Covid AusterityDocument8 paginiFin - e - 178 - 2022-Covid AusterityMARUTHUPANDIÎncă nu există evaluări
- Unit Test 9 BDocument1 paginăUnit Test 9 BAnnaÎncă nu există evaluări
- Downloaded From Manuals Search EngineDocument29 paginiDownloaded From Manuals Search EnginehaivermelosantanderÎncă nu există evaluări
- 10 Ideas For ConversationDocument116 pagini10 Ideas For ConversationGreenLake36100% (1)
- Metsec Steel Framing SystemDocument46 paginiMetsec Steel Framing Systemleonil7Încă nu există evaluări
- JBL Tune 115TWS HeadphoneDocument2 paginiJBL Tune 115TWS HeadphoneTimiÎncă nu există evaluări
- Bus Terminal Building AreasDocument3 paginiBus Terminal Building AreasRohit Kashyap100% (1)
- Petitioner vs. vs. Respondents Nicanor S. Bautista Agaton D. Yaranon Bince, Sevilleja, Agsalud & AssociatesDocument9 paginiPetitioner vs. vs. Respondents Nicanor S. Bautista Agaton D. Yaranon Bince, Sevilleja, Agsalud & AssociatesBianca BÎncă nu există evaluări
- BBC Focus - Answers To Lifes Big Questions 2017Document100 paginiBBC Focus - Answers To Lifes Big Questions 2017AD StrategoÎncă nu există evaluări
- H.P. Elementary Education Code Chapter - 4 - 2012 SMC by Vijay Kumar HeerDocument7 paginiH.P. Elementary Education Code Chapter - 4 - 2012 SMC by Vijay Kumar HeerVIJAY KUMAR HEERÎncă nu există evaluări
- Financial Management Full Notes at Mba FinanceDocument44 paginiFinancial Management Full Notes at Mba FinanceBabasab Patil (Karrisatte)86% (7)