S-ar putea să vă placă și
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- 5 Host Defense MechanismDocument62 pagini5 Host Defense MechanismAinaB ManaloÎncă nu există evaluări
- Immunology - 1200Document2.640 paginiImmunology - 1200tcabanilÎncă nu există evaluări
- Swine Diagnostic ManualDocument40 paginiSwine Diagnostic ManualSilvia DeaconuÎncă nu există evaluări
- Inprocess Quality Control Tests For Biological ProductsDocument34 paginiInprocess Quality Control Tests For Biological ProductsnishathfathimaÎncă nu există evaluări
- 20 Uses of Vicks VaporubDocument3 pagini20 Uses of Vicks VaporubDrBertram ForerÎncă nu există evaluări
- EQAS General InformationDocument13 paginiEQAS General Informationtanguy_chau100% (1)
- Budget Plan Wound ClinicDocument4 paginiBudget Plan Wound ClinicRegalado Aguhayon100% (1)
- NCP - Risk For InfectionDocument3 paginiNCP - Risk For InfectionSiergs Smith Gervacio100% (3)
- S AureusDocument2 paginiS AureusNina VeniaÎncă nu există evaluări
- ATTAR49Document10 paginiATTAR49vlande897Încă nu există evaluări
- Review Flash Card by Dr. Mitch Roy MaristelaDocument205 paginiReview Flash Card by Dr. Mitch Roy MaristelaMark Justin OcampoÎncă nu există evaluări
- Evidence Over Hysteria - COVID-19 - Six Four Six Nine - MediumDocument36 paginiEvidence Over Hysteria - COVID-19 - Six Four Six Nine - MediumDorian GrayÎncă nu există evaluări
- BacteriologyDocument14 paginiBacteriologysilcmtgÎncă nu există evaluări
- Biology Questions CholeraDocument12 paginiBiology Questions CholeraLucas100% (1)
- Paediatric History and Examination 08092012-2Document10 paginiPaediatric History and Examination 08092012-2Shahin KazemzadehÎncă nu există evaluări
- Upper Respiratory Tract InfectionDocument45 paginiUpper Respiratory Tract InfectionNatasha Abdulla100% (2)
- Approach To GI DisordersDocument28 paginiApproach To GI DisordersdrvivekshimlaÎncă nu există evaluări
- Guillain-Barre Syndrome: Practice EssentialsDocument16 paginiGuillain-Barre Syndrome: Practice EssentialsUKMBasketÎncă nu există evaluări
- Natural ImmunityDocument34 paginiNatural ImmunitySelvaram SelvaÎncă nu există evaluări
- Feline Infectious PeritonitisDocument59 paginiFeline Infectious PeritonitisBeda Meda100% (1)
- CPC Acute AppendicitisDocument57 paginiCPC Acute AppendicitisYS Nate100% (1)
- Evolution of Human Diseases - HO Smail PDFDocument17 paginiEvolution of Human Diseases - HO Smail PDFdoeditÎncă nu există evaluări
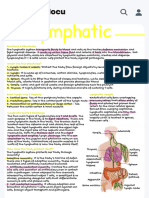
- Handwritten Lympathic - Functions & Structures The Lymphatic System Transports Fluids To Blood - StudocuDocument1 paginăHandwritten Lympathic - Functions & Structures The Lymphatic System Transports Fluids To Blood - StudocuAllyssa MarieÎncă nu există evaluări
- Science - November 7, 2014Document140 paginiScience - November 7, 2014Nicoleta Andreea TudoseÎncă nu există evaluări
- Assessment of The Implementation of Expanded Program On Immunization in Barangay Maranding, Lala, Lanao Del Norte From 2014-2018Document15 paginiAssessment of The Implementation of Expanded Program On Immunization in Barangay Maranding, Lala, Lanao Del Norte From 2014-2018Diana Grace ViñaÎncă nu există evaluări
- IspaDocument30 paginiIspahary anggoroÎncă nu există evaluări
- Therapeutically Administered Ribonucleoside Analogue Mk-4482/Eidd-2801 Blocks Sars-Cov-2 Transmission in FerretsDocument15 paginiTherapeutically Administered Ribonucleoside Analogue Mk-4482/Eidd-2801 Blocks Sars-Cov-2 Transmission in FerretsCarlosgustavo SaavedrarubioÎncă nu există evaluări
- Banana ResearchDocument14 paginiBanana ResearchJas TeshÎncă nu există evaluări
- A Mass Burial From The Cemetery of KerameikosDocument15 paginiA Mass Burial From The Cemetery of KerameikosLudwigRoss100% (1)
- Abstract Safety Endorsement - SMDocument5 paginiAbstract Safety Endorsement - SMapi-452651338Încă nu există evaluări