S-ar putea să vă placă și
- Psychomotor Skills Activity On Parenteral Routes of Drug AdministrationDocument15 paginiPsychomotor Skills Activity On Parenteral Routes of Drug AdministrationEmerson QuimbaÎncă nu există evaluări
- Medication Administration (Guide)Document6 paginiMedication Administration (Guide)Alane MorenoÎncă nu există evaluări
- Selection of Equipment and Administration of InjectionsDocument67 paginiSelection of Equipment and Administration of InjectionsSudhadKÎncă nu există evaluări
- Aspirating Drugs From Ampules and VialsDocument9 paginiAspirating Drugs From Ampules and VialsmariallenÎncă nu există evaluări
- Administration of Parenteral MedicationsDocument6 paginiAdministration of Parenteral Medicationsjoel david knda mjÎncă nu există evaluări
- Checklist of IM InjectionDocument5 paginiChecklist of IM InjectionSharon LawrenceÎncă nu există evaluări
- Administering Medications via TubeDocument16 paginiAdministering Medications via TubeYep YepÎncă nu există evaluări
- Obat Injeksi Parenteral AdministrationDocument43 paginiObat Injeksi Parenteral Administrationlistya dewiÎncă nu există evaluări
- Im Self InjectionDocument9 paginiIm Self InjectionInc hrgÎncă nu există evaluări
- Subkutan InjeksiDocument5 paginiSubkutan InjeksiAnggrian Clara DewiÎncă nu există evaluări
- Intramuscular Injection: 1-DefinitionDocument11 paginiIntramuscular Injection: 1-DefinitionkingÎncă nu există evaluări
- Parenteral Medication AdministrationDocument19 paginiParenteral Medication AdministrationMadhavi ModaÎncă nu există evaluări
- Withdrawing Medication From An Ampule: EquipmentDocument6 paginiWithdrawing Medication From An Ampule: EquipmentMj Andayog100% (1)
- Giving Subcutaneous InjectionsDocument6 paginiGiving Subcutaneous Injectionsmushroom620Încă nu există evaluări
- Finals Pharmaco LabDocument24 paginiFinals Pharmaco LabAubrey Nicole MacapagalÎncă nu există evaluări
- Parenteral Doasge Forms-1Document8 paginiParenteral Doasge Forms-1vikilsoni2Încă nu există evaluări
- IM Injuction: Definition of Intramuscular InjectionDocument8 paginiIM Injuction: Definition of Intramuscular InjectiondhanasundariÎncă nu există evaluări
- Year I Basic NursingDocument99 paginiYear I Basic Nursingmbok diyirÎncă nu există evaluări
- Administering Intravenous (IV) Medication - OSCE Guide - Geeky MedicsDocument7 paginiAdministering Intravenous (IV) Medication - OSCE Guide - Geeky MedicslortifukkuÎncă nu există evaluări
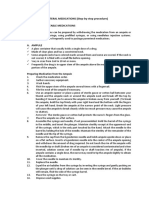
- Parenteral Medication Step by Step ProcedureDocument8 paginiParenteral Medication Step by Step ProcedureAubrey De GraciaÎncă nu există evaluări
- Med Admin ChecklistDocument9 paginiMed Admin ChecklistLoren MisticaÎncă nu există evaluări
- SRM I Year I Basic NursingDocument97 paginiSRM I Year I Basic Nursingmbok diyirÎncă nu există evaluări
- Care of Mother and Child Nursing ModuleDocument37 paginiCare of Mother and Child Nursing ModuleFregen Mae ApoyaÎncă nu există evaluări
- Administering Subcutaneous InjectionDocument6 paginiAdministering Subcutaneous InjectionAnggrian Clara DewiÎncă nu există evaluări
- Chapter 64 - Administration of Injectable MedicationsDocument11 paginiChapter 64 - Administration of Injectable Medicationskristie donaldÎncă nu există evaluări
- Withdrawing and Reconstituting MedicationsDocument6 paginiWithdrawing and Reconstituting MedicationsMelchizedek Tagarino TorioÎncă nu există evaluări
- Giving Subcutaneous InjectionDocument6 paginiGiving Subcutaneous Injection100WejdanÎncă nu există evaluări
- IntramuscularDocument4 paginiIntramusculargaatgaatÎncă nu există evaluări
- Administering Intradermal InjectionDocument17 paginiAdministering Intradermal InjectionPattÎncă nu există evaluări
- English Paper Injuction: Akper Bina Insani Sakti Sungai Penuh Tahun AJARAN 2020/2021Document10 paginiEnglish Paper Injuction: Akper Bina Insani Sakti Sungai Penuh Tahun AJARAN 2020/2021foelsi khasafutriÎncă nu există evaluări
- Intravena InjectionDocument6 paginiIntravena InjectionEvoLetd'LeenÎncă nu există evaluări
- Intra Muscular Injection in ChildrenDocument9 paginiIntra Muscular Injection in ChildrenssÎncă nu există evaluări
- IM Injection DemonstrationDocument13 paginiIM Injection DemonstrationMegha lakra100% (1)
- Ward 29 Guide To The Safe Preparation and Administration of Intravenous (IV) Antibiotics at HomeDocument18 paginiWard 29 Guide To The Safe Preparation and Administration of Intravenous (IV) Antibiotics at HomeSebut Saja MawarÎncă nu există evaluări
- Parenteral Routes of Administration&Dosage FormsDocument8 paginiParenteral Routes of Administration&Dosage FormsSonal SoniÎncă nu există evaluări
- Administering IntradermalDocument28 paginiAdministering IntradermalSaul Remus Q. DasmariñasÎncă nu există evaluări
- Subcutaneous InjectionDocument5 paginiSubcutaneous InjectionNovita sariÎncă nu există evaluări
- Preparation of Medication From Vial and AmpuleDocument9 paginiPreparation of Medication From Vial and AmpulePATRICIA JULIANNE CASTAÑETO RIVERAÎncă nu există evaluări
- Administering Intramuscular InjectionDocument7 paginiAdministering Intramuscular Injectionthanuja mathew100% (1)
- Withdrawing Medication From An AmpuleDocument7 paginiWithdrawing Medication From An AmpuleJisha JanardhanÎncă nu există evaluări
- IM InjectionDocument4 paginiIM InjectionAdrija SenÎncă nu există evaluări
- 2 Intramuscular InjectionDocument5 pagini2 Intramuscular InjectionKEANNA ZURRIAGAÎncă nu există evaluări
- Administering An IntradermalDocument7 paginiAdministering An IntradermalCzarina Mae Quinones TadeoÎncă nu există evaluări
- Misamis University: Administering Parenteral MedicationsDocument10 paginiMisamis University: Administering Parenteral MedicationsAkio OzaragaÎncă nu există evaluări
- IV InjectionDocument10 paginiIV Injectionpreeti sharmaÎncă nu există evaluări
- IntradermalDocument7 paginiIntradermalKyle Dapulag100% (1)
- GuidesDocument10 paginiGuidesJClaudz PilapilÎncă nu există evaluări
- Observation Competence Checklist For Administration of An Intramuscular InjectionDocument24 paginiObservation Competence Checklist For Administration of An Intramuscular InjectionNada S'jÎncă nu există evaluări
- IMself Injection TDocument5 paginiIMself Injection TLamettaÎncă nu există evaluări
- PDF 1Document101 paginiPDF 1Ma. Ferimi Gleam BajadoÎncă nu există evaluări
- A Brief History of the SyringeDocument7 paginiA Brief History of the Syringeeloie100% (1)
- 14B Preparing Medications From VialsDocument4 pagini14B Preparing Medications From VialsMarky RoqueÎncă nu există evaluări
- How to Give an Intramuscular Injection SafelyDocument17 paginiHow to Give an Intramuscular Injection SafelyArunesh 456100% (1)
- Drug Preparation: (Ampule and Vial)Document25 paginiDrug Preparation: (Ampule and Vial)Ron Lucernas MayugaÎncă nu există evaluări
- Proper Medication Preparation from Ampules and VialsDocument2 paginiProper Medication Preparation from Ampules and VialsthadzamingÎncă nu există evaluări
- How to Give an Injection SafelyDocument2 paginiHow to Give an Injection SafelyLiza AryaniÎncă nu există evaluări
- Intravenous and Intramuscular InjectionsDocument12 paginiIntravenous and Intramuscular Injectionsshubham rathodÎncă nu există evaluări
- DateDocument4 paginiDateAbby Trisha MadularaÎncă nu există evaluări
- Injection TechniquesDocument11 paginiInjection TechniquesLeon OngÎncă nu există evaluări
- A Simple Guide To Emergency Tips And Improvised Health CareDe la EverandA Simple Guide To Emergency Tips And Improvised Health CareÎncă nu există evaluări
- PCL S PDFDocument1 paginăPCL S PDFspectre68Încă nu există evaluări
- Environmental Engineering Test PaperDocument16 paginiEnvironmental Engineering Test PaperajaydevmalikÎncă nu există evaluări
- Nutrition Therapy For Adults With Diabetes or Prediabetes A Consensus Report - 2019 PDFDocument24 paginiNutrition Therapy For Adults With Diabetes or Prediabetes A Consensus Report - 2019 PDFNicolás Di SantoroÎncă nu există evaluări
- Schilders PDFDocument3 paginiSchilders PDFStefania FloreaÎncă nu există evaluări
- Clinical Digital Photography in OrthodonticsDocument67 paginiClinical Digital Photography in OrthodonticsLivia MarianaÎncă nu există evaluări
- Cardiogenic ShockDocument42 paginiCardiogenic ShockpashaÎncă nu există evaluări
- Top 3 Nursing Care PlanDocument3 paginiTop 3 Nursing Care PlanAC TamayoÎncă nu există evaluări
- OrthodonticsThe Role of Removable Appliances in CoDocument6 paginiOrthodonticsThe Role of Removable Appliances in Cokakanya donghyukÎncă nu există evaluări
- Homeopatija I AstmaDocument10 paginiHomeopatija I AstmaBranka PopovicÎncă nu există evaluări
- Diabetic Ketoacidosis and Respiratory CompensationDocument3 paginiDiabetic Ketoacidosis and Respiratory CompensationcpccoderÎncă nu există evaluări
- Applied Social Psychology Module 2Document5 paginiApplied Social Psychology Module 2swathy sudheerÎncă nu există evaluări
- Causes, Workup and Management of Epistaxis: AssignmentDocument4 paginiCauses, Workup and Management of Epistaxis: AssignmentFarhan AfzalÎncă nu există evaluări
- Chapter 60: Headache: Section 10: NeurologyDocument16 paginiChapter 60: Headache: Section 10: NeurologyAnonymous Xmb6QQvRÎncă nu există evaluări
- Guidelines Textile Industry Draft PDFDocument36 paginiGuidelines Textile Industry Draft PDFRohan LadÎncă nu există evaluări
- Antepartum HaemorrhageDocument18 paginiAntepartum HaemorrhageOjambo Flavia100% (1)
- What Are Anxiety Disorders/depressions?Document2 paginiWhat Are Anxiety Disorders/depressions?Cams BlogÎncă nu există evaluări
- NURS 6521 Final Exam Study GuideDocument3 paginiNURS 6521 Final Exam Study GuideTracy MÎncă nu există evaluări
- Hinshaw, 1992. Academic Underachievement, Attention Deficits, and Aggression. Comorbidity and Implications For InterventionDocument11 paginiHinshaw, 1992. Academic Underachievement, Attention Deficits, and Aggression. Comorbidity and Implications For InterventionManuel José Serafin PlasenciaÎncă nu există evaluări
- Trauma and Recovery PrimerDocument15 paginiTrauma and Recovery Primershperka100% (1)
- Tooth Discoloration and HomoeopathyDocument12 paginiTooth Discoloration and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- InfidelityDocument18 paginiInfidelityGeorgiana GattinaÎncă nu există evaluări
- Trabeculectomy-Related Corneal ComplicationsDocument7 paginiTrabeculectomy-Related Corneal ComplicationsDian Putri NingsihÎncă nu există evaluări
- Recovery of Glycerine From Spent Palm Kernel Soap and Palm Oil Soap LyeDocument8 paginiRecovery of Glycerine From Spent Palm Kernel Soap and Palm Oil Soap LyeNadya Larasati KrdÎncă nu există evaluări
- Gastric and Duodenal Disorders - Test 4Document21 paginiGastric and Duodenal Disorders - Test 4Vickie BuckerÎncă nu există evaluări
- NCP FinalDocument18 paginiNCP FinalJessica Medina100% (1)
- Organizational Behavior: Stephen P. RobbinsDocument24 paginiOrganizational Behavior: Stephen P. Robbinskria1167% (3)
- Case Presentation LM PotencyDocument33 paginiCase Presentation LM PotencyVaseem Azizii100% (3)
- Enc of FibromyalgiaDocument214 paginiEnc of Fibromyalgiadeb4paul100% (3)
- Tarpan Therapy A Potential Ocular Therapeutics in AyurvedaDocument3 paginiTarpan Therapy A Potential Ocular Therapeutics in AyurvedaBozidar MicicÎncă nu există evaluări
- Cesarean Section in A MareDocument26 paginiCesarean Section in A MareSERGIO ALEJANDRO CARDENAS ALDANAÎncă nu există evaluări