S-ar putea să vă placă și
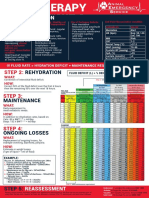
- AES - FluidChart 2020Document1 paginăAES - FluidChart 2020Christian De Leon100% (1)
- Hematological Disorders of NewbornDocument98 paginiHematological Disorders of Newbornlieynna499650% (2)
- Veterinary Internal Medicne - 2008 - Bruchim - Heat Stroke in Dogs A Retrospective Study of 54 Cases 1999 2004 andDocument9 paginiVeterinary Internal Medicne - 2008 - Bruchim - Heat Stroke in Dogs A Retrospective Study of 54 Cases 1999 2004 andGuillermo MuzasÎncă nu există evaluări
- M. Tuberculosis, M. Bovis, M. Microti, M. Canettii, M. Africanum, and M. PinnipediiDocument5 paginiM. Tuberculosis, M. Bovis, M. Microti, M. Canettii, M. Africanum, and M. PinnipediiSurya Wahyu NugrohoÎncă nu există evaluări
- PanosteitisDocument5 paginiPanosteitisUmesh GopalanÎncă nu există evaluări
- Timoma em Coelhos - Sinais Clínicos, Diagnóstico, Tratamento PDFDocument8 paginiTimoma em Coelhos - Sinais Clínicos, Diagnóstico, Tratamento PDFRenata MateusÎncă nu există evaluări
- Babapulle 1993Document10 paginiBabapulle 1993javier reyÎncă nu există evaluări
- Case ReportDocument4 paginiCase ReportbejoÎncă nu există evaluări
- LP DHFDocument17 paginiLP DHFAfif SubhanÎncă nu există evaluări
- Toad Poisoning in Three Dogs: Case Reports: February 10, 2009 July 29, 2009 September 14, 2009 November 30, 2009Document10 paginiToad Poisoning in Three Dogs: Case Reports: February 10, 2009 July 29, 2009 September 14, 2009 November 30, 2009ivanacrisÎncă nu există evaluări
- A33v35n4 PDFDocument4 paginiA33v35n4 PDFAnonymous GzRz4H50FÎncă nu există evaluări
- Van Buchem DiseaseDocument9 paginiVan Buchem DiseaseZehra UrunÎncă nu există evaluări
- A Case of Canine Trypanosomosis With Epistaxis in A TwoYear Old Alsatian DogDocument5 paginiA Case of Canine Trypanosomosis With Epistaxis in A TwoYear Old Alsatian DogIOSRjournalÎncă nu există evaluări
- Infection With Anaplasma Phagocytophilum in A Young Dog: A Case ReportDocument6 paginiInfection With Anaplasma Phagocytophilum in A Young Dog: A Case Reportcicelynara94Încă nu există evaluări
- Botryoid Nuclei in The Peripheral Blood of A Dog With HeatstrokeDocument5 paginiBotryoid Nuclei in The Peripheral Blood of A Dog With HeatstrokeLaboratorio de BioquimicaÎncă nu există evaluări
- Estimating The Outcome of Umbilical Diseases Based On Clinical Examination in Calves: 322 CasesDocument5 paginiEstimating The Outcome of Umbilical Diseases Based On Clinical Examination in Calves: 322 CasesFathurrahman Maulana RifqiÎncă nu există evaluări
- Thermographic Imaging in A Dog With Macroglossia From An Encircling, Strangulating Lingual Linear Foreign BodyDocument4 paginiThermographic Imaging in A Dog With Macroglossia From An Encircling, Strangulating Lingual Linear Foreign BodyFrancisco Luis Briseño MedinaÎncă nu există evaluări
- Bite Wounds Involving The Spine Characteristics Therapy and Outcome in Seven CasesDocument7 paginiBite Wounds Involving The Spine Characteristics Therapy and Outcome in Seven CasesbiasbsanÎncă nu există evaluări
- Feline Idiopathic Cardiomyopathy: A Retrospective Study of 106 Cats (1994-2001)Document9 paginiFeline Idiopathic Cardiomyopathy: A Retrospective Study of 106 Cats (1994-2001)Carol Mitie TamuraÎncă nu există evaluări
- Nitric Oxide and Prostaglandins - Important Players in Endothelin-1 Induced Myocardial DistensibilityDocument10 paginiNitric Oxide and Prostaglandins - Important Players in Endothelin-1 Induced Myocardial DistensibilityZamfir CorneliuÎncă nu există evaluări
- Morphological Changes in Blood Cells in A Rat Model of Heatstroke: A Pilot StudyDocument13 paginiMorphological Changes in Blood Cells in A Rat Model of Heatstroke: A Pilot StudyDaniel Roberto Sáenz GarcíaÎncă nu există evaluări
- HAEMANGIOSARCOMA in DOGSDocument11 paginiHAEMANGIOSARCOMA in DOGSPdea CanineÎncă nu există evaluări
- Descricion ofDocument5 paginiDescricion ofLlrss AdnÎncă nu există evaluări
- Thymic LymphDocument7 paginiThymic LymphMaxim AlmousaÎncă nu există evaluări
- Canine and Feline Intracraneal Meningiomas, An Update ReviexDocument13 paginiCanine and Feline Intracraneal Meningiomas, An Update ReviexFelipe GonzalezÎncă nu există evaluări
- A Procedure For Creating A Frailty Index Based On Deficis in Mice - Parks - 2012Document11 paginiA Procedure For Creating A Frailty Index Based On Deficis in Mice - Parks - 2012gon71Încă nu există evaluări
- USPancreas DR GomaaDocument14 paginiUSPancreas DR GomaaFlavio RibeiroÎncă nu există evaluări
- HomeostasisDocument2 paginiHomeostasisImelda Verawaty Lumban GaolÎncă nu există evaluări
- Hyper Tak NgaruhDocument10 paginiHyper Tak NgaruhNouchan NoupÎncă nu există evaluări
- s13620 014 0028 8 PDFDocument9 paginis13620 014 0028 8 PDFdewaÎncă nu există evaluări
- Heng 2017Document6 paginiHeng 2017CLINICA VETERINARIA DE MEDELLINÎncă nu există evaluări
- A Case Report of Feline Pituitary Carcinoma With HypercortisolismDocument6 paginiA Case Report of Feline Pituitary Carcinoma With HypercortisolismSatriaÎncă nu există evaluări
- A Retrospective Histopathological Survey On Canine and Feline Liver Diseases at The University of Tokyo Between 2006 and 2012Document6 paginiA Retrospective Histopathological Survey On Canine and Feline Liver Diseases at The University of Tokyo Between 2006 and 2012Flaviu TabaranÎncă nu există evaluări
- Heat Stroke in DogsDocument8 paginiHeat Stroke in DogsScott ReedÎncă nu există evaluări
- Hydro CardiovasDocument39 paginiHydro CardiovasFransiskus Xaverius CungkringÎncă nu există evaluări
- A Retrospective Study of Cardiac Hemangiosarcoma in DogsDocument5 paginiA Retrospective Study of Cardiac Hemangiosarcoma in DogsDzulfikarFaizinRomasÎncă nu există evaluări
- Sabevetal PDFDocument5 paginiSabevetal PDFDimas MedelluÎncă nu există evaluări
- Diagnostic Dilemma of Sudden Deaths Due To Acute Hemorrhagic PancreatitisDocument3 paginiDiagnostic Dilemma of Sudden Deaths Due To Acute Hemorrhagic PancreatitisM25 BhayangkaraÎncă nu există evaluări
- Pulmonary Pathological Features in Coronavirus Associated Severe Acute Respiratory Syndrome (SARS)Document6 paginiPulmonary Pathological Features in Coronavirus Associated Severe Acute Respiratory Syndrome (SARS)Leandro VillamilÎncă nu există evaluări
- Shivering Thermogenesis in Humans Origin, Contribution and MetabolicDocument10 paginiShivering Thermogenesis in Humans Origin, Contribution and MetabolicGio VandaÎncă nu există evaluări
- Integumentary System: Cytology & HistologyDocument11 paginiIntegumentary System: Cytology & HistologyHelen ShuangÎncă nu există evaluări
- Clinico Diagnostic Studies On Traumatic Reticulopericarditis in Cattle - A Review of 56 CasesDocument11 paginiClinico Diagnostic Studies On Traumatic Reticulopericarditis in Cattle - A Review of 56 CasesSasikala KaliapanÎncă nu există evaluări
- Ijvm June 2011 FinalDocument64 paginiIjvm June 2011 FinalAmitesh DubeyÎncă nu există evaluări
- Casos Clínicos: Revista Colombiana de Ciencias PecuariasDocument7 paginiCasos Clínicos: Revista Colombiana de Ciencias PecuariasDharma AudiaÎncă nu există evaluări
- Traumaticpericarditisinbuffaloes MohamedDocument7 paginiTraumaticpericarditisinbuffaloes MohamedAnggun PutriÎncă nu există evaluări
- CO Inhalation at Dose Corresponding To Tobacco Smoke Worsens Cardiac Remodeling After Experimental Myocardial Infarction in RatsDocument7 paginiCO Inhalation at Dose Corresponding To Tobacco Smoke Worsens Cardiac Remodeling After Experimental Myocardial Infarction in RatsGael ROCHEFORTÎncă nu există evaluări
- Where Hypertension Happens: CommentariesDocument4 paginiWhere Hypertension Happens: CommentariesIlvita MayasariÎncă nu există evaluări
- Weil Et Al NoD 2009Document9 paginiWeil Et Al NoD 2009zacharymweilÎncă nu există evaluări
- Hepatic Echinococcus Granulosus. A Case ReportDocument2 paginiHepatic Echinococcus Granulosus. A Case ReportIngrid DuarteÎncă nu există evaluări
- Toxicopathological Effects of Intravenous Injection of Layer Double Hydroxide (LDH) Nanoparticles in Male Rats.Document16 paginiToxicopathological Effects of Intravenous Injection of Layer Double Hydroxide (LDH) Nanoparticles in Male Rats.Amar AmarÎncă nu există evaluări
- Death Death: - Defined As Cessation of Life Ie Total Stoppage of Blood Circulation and ADocument10 paginiDeath Death: - Defined As Cessation of Life Ie Total Stoppage of Blood Circulation and APrashant MeenaÎncă nu există evaluări
- Spontaneous Hemopneumothorax: A Rare But Life-Threatening EntityDocument4 paginiSpontaneous Hemopneumothorax: A Rare But Life-Threatening EntityCornelia LongginuzÎncă nu există evaluări
- Echografische en Radiografische Abnormaliteiten in de Nieren Van Zes Honden en Een Kat Met EthyleenglycolintoxicatieDocument9 paginiEchografische en Radiografische Abnormaliteiten in de Nieren Van Zes Honden en Een Kat Met EthyleenglycolintoxicatiedpcamposhÎncă nu există evaluări
- Artículo 2Document5 paginiArtículo 2Marco Rodríguez JiménezÎncă nu există evaluări
- DRESS Syndrome in A Patient On Sulfasalazine For Rheumatoid ArthritisDocument4 paginiDRESS Syndrome in A Patient On Sulfasalazine For Rheumatoid ArthritisChistian LassoÎncă nu există evaluări
- BOTSCH 2009 Retrospective Study of Dogs With ThrombocytopeniaDocument5 paginiBOTSCH 2009 Retrospective Study of Dogs With ThrombocytopeniaElle Burton-BradleyÎncă nu există evaluări
- Henry Ford Hospital Medical Journal Henry Ford Hospital Medical JournalDocument8 paginiHenry Ford Hospital Medical Journal Henry Ford Hospital Medical JournalIrsalina SalmaÎncă nu există evaluări
- Artigo ParasitariasDocument5 paginiArtigo Parasitariasdanex.marquesÎncă nu există evaluări
- Neurohormonal Activation in Severe Scorpion Envenomation: Correlation With Hemodynamics and Circulating ToxinDocument6 paginiNeurohormonal Activation in Severe Scorpion Envenomation: Correlation With Hemodynamics and Circulating ToxinDaniela SalamancaÎncă nu există evaluări
- Hard AwayDocument4 paginiHard AwayEdmund Ocado JrÎncă nu există evaluări
- Of The Entire Family Died: Many Have Been Widowed: and Many of The Survivors AreDocument8 paginiOf The Entire Family Died: Many Have Been Widowed: and Many of The Survivors ArebhaktispÎncă nu există evaluări
- Thyroiditis and Thyroid Function: Clinical, Morphological, and Physiopathological StudiesDe la EverandThyroiditis and Thyroid Function: Clinical, Morphological, and Physiopathological StudiesÎncă nu există evaluări
- 2020 July Egg Transfer Scott MartinDocument70 pagini2020 July Egg Transfer Scott MartinChristian De LeonÎncă nu există evaluări
- Glycogen Isolation and Determination ofDocument14 paginiGlycogen Isolation and Determination ofChristian De LeonÎncă nu există evaluări
- Flores - TVTDocument9 paginiFlores - TVTChristian De LeonÎncă nu există evaluări
- Lobetti - Ivermectin ToxicityDocument3 paginiLobetti - Ivermectin ToxicityChristian De LeonÎncă nu există evaluări
- Chervier - FeverDocument4 paginiChervier - FeverChristian De LeonÎncă nu există evaluări
- PB - Evaluative Exam 4QDocument15 paginiPB - Evaluative Exam 4QAnnizaÎncă nu există evaluări
- Hypoxic Ischemic Encephalopathy (Hie) : AlgorithmDocument11 paginiHypoxic Ischemic Encephalopathy (Hie) : Algorithmsidharth sauravÎncă nu există evaluări
- Koagulasi Intravaskuler Diseminata Pada Kanker: January 2015Document13 paginiKoagulasi Intravaskuler Diseminata Pada Kanker: January 2015Sri IriantiÎncă nu există evaluări
- Pancreatitis Diabetes GatosDocument15 paginiPancreatitis Diabetes GatosMónica CalviñoÎncă nu există evaluări
- Postpartum HemorrhageDocument22 paginiPostpartum HemorrhageReynaldiReikyHadiwijayaÎncă nu există evaluări
- NCLEX Questions OB QuestionsDocument4 paginiNCLEX Questions OB QuestionsAlvin L. Rozier100% (1)
- Complications Blood TransfusionDocument7 paginiComplications Blood TransfusionWajeehaWasimÎncă nu există evaluări
- Pre Gestational ConditionsDocument68 paginiPre Gestational ConditionsQuinonez Anna MarieÎncă nu există evaluări
- PBM Module1 MTP Template 0Document2 paginiPBM Module1 MTP Template 01234chocoÎncă nu există evaluări
- Sepsis: Sepsis and Septic ShockDocument22 paginiSepsis: Sepsis and Septic ShockWialda Dwi rodyahÎncă nu există evaluări
- Gastric Dilation-Volvulus Syndrome in Dogs 2. Surgical and Postoperative ManagementDocument8 paginiGastric Dilation-Volvulus Syndrome in Dogs 2. Surgical and Postoperative ManagementThiara Ayu PangestiÎncă nu există evaluări
- Nursing Clients With Hematologic DisordersDocument4 paginiNursing Clients With Hematologic DisordersLuna MarieÎncă nu există evaluări
- C-2 Operators Manual V11.15Document61 paginiC-2 Operators Manual V11.15Oana NedelcuÎncă nu există evaluări
- COVID-19 Preventive Behaviors and Influencing Factors in The Iranian Population A Web-Based SurveyDocument7 paginiCOVID-19 Preventive Behaviors and Influencing Factors in The Iranian Population A Web-Based SurveyAsti YumnaÎncă nu există evaluări
- Cheat Sheet #92 - Disseminated Intravascular CoaguationDocument3 paginiCheat Sheet #92 - Disseminated Intravascular CoaguationAsssÎncă nu există evaluări
- Leg Med Cases For MidtermsDocument154 paginiLeg Med Cases For MidtermsJae LeeÎncă nu există evaluări
- Prof - Mansyur Arief - Peran Pemeriksaan HematologiDocument30 paginiProf - Mansyur Arief - Peran Pemeriksaan HematologiRahmawati RusmanÎncă nu există evaluări
- HRM Week 2 - Introduction 2020 - PrintDocument34 paginiHRM Week 2 - Introduction 2020 - PrintShiv SookunÎncă nu există evaluări
- Postpartum ComplicationsDocument42 paginiPostpartum ComplicationsElvisÎncă nu există evaluări
- MeltdownDocument92 paginiMeltdownMyles SamÎncă nu există evaluări
- Opm M2 V117UV EN Rev11Document58 paginiOpm M2 V117UV EN Rev11Jose Rolando Orellana Rodriguez0% (1)
- Blood and Its ComponentsDocument30 paginiBlood and Its ComponentskushalÎncă nu există evaluări
- @MBS MedicalBooksStore 2020 CompressionDocument46 pagini@MBS MedicalBooksStore 2020 CompressionTaufikÎncă nu există evaluări
- Overview SepsisDocument13 paginiOverview SepsisYanna RizkiaÎncă nu există evaluări
- Canine & Feline CoagulopathyDocument6 paginiCanine & Feline CoagulopathyJovana SmiljanićÎncă nu există evaluări
- Polycythemia: (Primary & Secondary)Document16 paginiPolycythemia: (Primary & Secondary)Vanessa Camille DomingoÎncă nu există evaluări
- Routine Use of Vitamin K in The Treatment of Cirrhosis-Related Coagulopathy: Is It A-O-K? Maybe Not, We SayDocument6 paginiRoutine Use of Vitamin K in The Treatment of Cirrhosis-Related Coagulopathy: Is It A-O-K? Maybe Not, We Sayannisa edwarÎncă nu există evaluări
- JTH 14015Document4 paginiJTH 14015Catherine MorrisÎncă nu există evaluări