S-ar putea să vă placă și
- Digital Health: Scaling Healthcare to the WorldDe la EverandDigital Health: Scaling Healthcare to the WorldHomero RivasÎncă nu există evaluări
- Religare Pre Auth FormDocument3 paginiReligare Pre Auth FormM/s Microtech25% (4)
- Cross-Training: The Medical Assistant WorkbookDe la EverandCross-Training: The Medical Assistant WorkbookÎncă nu există evaluări
- Religare Claim FormDocument3 paginiReligare Claim FormTofan kumar MohapatraÎncă nu există evaluări
- Healthcare Information Technology for Cardiovascular Medicine: Telemedicine & Digital HealthDe la EverandHealthcare Information Technology for Cardiovascular Medicine: Telemedicine & Digital HealthAmi B. BhattÎncă nu există evaluări
- Preauth FormDocument3 paginiPreauth FormKunal JagnadeÎncă nu există evaluări
- Cashless Request FormDocument4 paginiCashless Request FormManish RanjanÎncă nu există evaluări
- Care For Vulnerable Populations during COVID-19 Pandemic: Clinical Updates in COVID-19De la EverandCare For Vulnerable Populations during COVID-19 Pandemic: Clinical Updates in COVID-19Încă nu există evaluări
- District Hospital Standards PDFDocument23 paginiDistrict Hospital Standards PDFsurbhi aggarwalÎncă nu există evaluări
- Bajaj Allianz Cashless Request FormDocument3 paginiBajaj Allianz Cashless Request FormM/s MicrotechÎncă nu există evaluări
- Medical FormDocument4 paginiMedical Formnki5Încă nu există evaluări
- Pre-Authorization Request Form: (Please Tick The Relevant Box)Document1 paginăPre-Authorization Request Form: (Please Tick The Relevant Box)Pallavi ShuklaÎncă nu există evaluări
- Accreditation OfferDocument14 paginiAccreditation Offeramira_hassan100% (1)
- Pages 5 Form FDocument2 paginiPages 5 Form FANIL KUMARÎncă nu există evaluări
- Application For Chief Minister Relief FundDocument5 paginiApplication For Chief Minister Relief FundVamsi KrishnaÎncă nu există evaluări
- 200 Bed Hospital Project ReportDocument40 pagini200 Bed Hospital Project Reportsaleha sultanaÎncă nu există evaluări
- QCIDocument27 paginiQCIerpÎncă nu există evaluări
- Application For Chief Minister Relief FundDocument5 paginiApplication For Chief Minister Relief FundVenkateswarlu ChennaiepalemÎncă nu există evaluări
- KPME Rules 2009Document46 paginiKPME Rules 2009Nausheen AnsariÎncă nu există evaluări
- Details of Primary Insured: Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part ADocument5 paginiDetails of Primary Insured: Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part ASumitThoratÎncă nu există evaluări
- Claim Form IHealthcareDocument5 paginiClaim Form IHealthcarePradeep Kumar VupalaÎncă nu există evaluări
- Raksha New Pre-Authorization FormDocument1 paginăRaksha New Pre-Authorization Formjigerpanchal0% (1)
- Nabh Application Dental ClinicDocument13 paginiNabh Application Dental ClinicPriya HariÎncă nu există evaluări
- 2017 Annual Hospital QuestionnaireDocument23 pagini2017 Annual Hospital QuestionnairebhagyaÎncă nu există evaluări
- Ayushman Bharat: Pradhan Mantri Jan Arogya YojanaDocument21 paginiAyushman Bharat: Pradhan Mantri Jan Arogya Yojana'Aakash Yadav'Încă nu există evaluări
- Sabari 200 Beded Hospital Project OfficeDocument40 paginiSabari 200 Beded Hospital Project OfficeGiridhari Prasad NayakÎncă nu există evaluări
- Health Act 2005 - 1Document24 paginiHealth Act 2005 - 1Anonymous jQwBrGlNGÎncă nu există evaluări
- Certificate ADocument4 paginiCertificate ASaurabh MehtaÎncă nu există evaluări
- Echs Sop PDFDocument39 paginiEchs Sop PDFnavneet baliÎncă nu există evaluări
- Application For Accreditation of ShcoDocument12 paginiApplication For Accreditation of ShcocrycardÎncă nu există evaluări
- Claims Reimbursement Form: Member General InformationDocument1 paginăClaims Reimbursement Form: Member General InformationFirmament DevelopmentÎncă nu există evaluări
- Form Med-97Document3 paginiForm Med-97ysraog5@yahoo.comÎncă nu există evaluări
- DH 201 To 300 Bedded Revised Draft PDFDocument158 paginiDH 201 To 300 Bedded Revised Draft PDFAmit Kumar MishraÎncă nu există evaluări
- MSO Citizen - CharterDocument7 paginiMSO Citizen - Chartersunshine7883Încă nu există evaluări
- Office Memorandum Dated 17.10Document21 paginiOffice Memorandum Dated 17.10Pradeep SaxenaÎncă nu există evaluări
- Annex e Hospital Stat Report Revised 7jan2014Document14 paginiAnnex e Hospital Stat Report Revised 7jan2014Andy Molina100% (1)
- Others Claim FormDocument5 paginiOthers Claim FormArvind RayÎncă nu există evaluări
- Obp PDFDocument39 paginiObp PDFBalhansÎncă nu există evaluări
- 2 - Hospital and It's Organization-1Document30 pagini2 - Hospital and It's Organization-1Qambar abbasÎncă nu există evaluări
- Rapid Hospital Readiness Checklist For Covid-19Document17 paginiRapid Hospital Readiness Checklist For Covid-19rommÎncă nu există evaluări
- Maxicare Reimbursement Claim Form PDFDocument1 paginăMaxicare Reimbursement Claim Form PDFJolina de VeraÎncă nu există evaluări
- Go Ms 38 Private Hospital Within and Outside State PDFDocument3 paginiGo Ms 38 Private Hospital Within and Outside State PDFsivaÎncă nu există evaluări
- WHO 2020 Covid19 BioEquip OpenDocument24 paginiWHO 2020 Covid19 BioEquip OpenDouglas RereseÎncă nu există evaluări
- Claims Reimbursement Form: Member General InformationDocument1 paginăClaims Reimbursement Form: Member General InformationHarold TanÎncă nu există evaluări
- Hospital Experiences Responding To The COVID-19 PandemicDocument41 paginiHospital Experiences Responding To The COVID-19 PandemicLaw&CrimeÎncă nu există evaluări
- Read HHS Inspector General's ReportDocument41 paginiRead HHS Inspector General's Reportkballuck1Încă nu există evaluări
- HHS Inspector General Report Covid 19 Oei-06!20!00300Document41 paginiHHS Inspector General Report Covid 19 Oei-06!20!00300Douglas PierreÎncă nu există evaluări
- Mou of Echs 2020-21Document10 paginiMou of Echs 2020-21SATYAM HOSPITALÎncă nu există evaluări
- Hamad - alhusaini@NHRA - BH Saad - rashed@NHRA - BH WWW - Nhra.bhDocument5 paginiHamad - alhusaini@NHRA - BH Saad - rashed@NHRA - BH WWW - Nhra.bhKazi MohammedÎncă nu există evaluări
- GSL BMW ApplDocument6 paginiGSL BMW ApplNANIBABUÎncă nu există evaluări
- Application For Registration/Renewal of Nursing Homes/Hospitals/ClinicsDocument8 paginiApplication For Registration/Renewal of Nursing Homes/Hospitals/Clinicsbalab2311Încă nu există evaluări
- APTRANSCO-Form of Application For Medical ClaimsDocument6 paginiAPTRANSCO-Form of Application For Medical ClaimsmastiÎncă nu există evaluări
- S.L Bello Maternity and Lying-In Clinic: Philippine Health Insurance CorporationDocument2 paginiS.L Bello Maternity and Lying-In Clinic: Philippine Health Insurance CorporationRose Bello-BersamiraÎncă nu există evaluări
- Format of Authorization Application For PHC and DispensaryDocument7 paginiFormat of Authorization Application For PHC and DispensaryRajat AroraÎncă nu există evaluări
- DH 301 To 500 Bedded Revised DraftDocument162 paginiDH 301 To 500 Bedded Revised Draftdemullu reddiÎncă nu există evaluări
- 3097693951-Guidelines For Setting Up of 10 Bedded AYUSH HospitalDocument10 pagini3097693951-Guidelines For Setting Up of 10 Bedded AYUSH Hospitalwk100% (1)
- Personal Accident'S / Accident Medical Reimbursement'S Attending Physician'S StatementDocument4 paginiPersonal Accident'S / Accident Medical Reimbursement'S Attending Physician'S Statementts8166Încă nu există evaluări
- FokodhariDocument355 paginiFokodhariGLOBOPOINT CONSULTANTSÎncă nu există evaluări
- Dashboard - Reveal Math, Grade 4 - McGraw HillDocument1 paginăDashboard - Reveal Math, Grade 4 - McGraw HillTijjani ShehuÎncă nu există evaluări
- WFM 5101 Watershed Hydrology: Shammi HaqueDocument18 paginiWFM 5101 Watershed Hydrology: Shammi HaquejahirÎncă nu există evaluări
- Honeywell Rondostat Hr20 SpesificationDocument2 paginiHoneywell Rondostat Hr20 Spesificationfrox123Încă nu există evaluări
- Work Permits New Guideline Amendments 2021 23.11.2021Document7 paginiWork Permits New Guideline Amendments 2021 23.11.2021Sabrina BrathwaiteÎncă nu există evaluări
- Science Grade 10 (Exam Prep)Document6 paginiScience Grade 10 (Exam Prep)Venice Solver100% (3)
- 50 Law-Firms Details by Vaibhav SharmaDocument17 pagini50 Law-Firms Details by Vaibhav SharmaApoorva NandiniÎncă nu există evaluări
- Course Outline Cbmec StratmgtDocument2 paginiCourse Outline Cbmec StratmgtskyieÎncă nu există evaluări
- Atoll 1400Document2 paginiAtoll 1400David M. SeoaneÎncă nu există evaluări
- IELTS Material Writing 1Document112 paginiIELTS Material Writing 1Lê hoàng anhÎncă nu există evaluări
- Altos Easystore Users ManualDocument169 paginiAltos Easystore Users ManualSebÎncă nu există evaluări
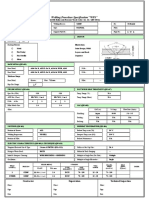
- Wps For Carbon Steel THK 7.11 GtawDocument1 paginăWps For Carbon Steel THK 7.11 GtawAli MoosaviÎncă nu există evaluări
- CO 101 Introductory Computing CO 102 Computing LabDocument17 paginiCO 101 Introductory Computing CO 102 Computing Labadityabaid4Încă nu există evaluări
- E-Waste: Name: Nishant.V.Naik Class: F.Y.Btech (Civil) Div: VII SR - No: 18 Roll No: A050136Document11 paginiE-Waste: Name: Nishant.V.Naik Class: F.Y.Btech (Civil) Div: VII SR - No: 18 Roll No: A050136Nishant NaikÎncă nu există evaluări
- Vertical Cutoff WallsDocument18 paginiVertical Cutoff WallsMark LaiÎncă nu există evaluări
- Ziarek - The Force of ArtDocument233 paginiZiarek - The Force of ArtVero MenaÎncă nu există evaluări
- M.Sc. Steel Structures LEC. #7 Plastic Analysis and Design: Dr. Qasim Shaukat KhanDocument43 paginiM.Sc. Steel Structures LEC. #7 Plastic Analysis and Design: Dr. Qasim Shaukat KhanSSÎncă nu există evaluări
- SAP HCM Case StudyDocument17 paginiSAP HCM Case StudyRafidaFatimatuzzahraÎncă nu există evaluări
- 1 s2.0 S2238785423001345 MainDocument10 pagini1 s2.0 S2238785423001345 MainHamada Shoukry MohammedÎncă nu există evaluări
- Walton Finance Way Strategy (MO)Document12 paginiWalton Finance Way Strategy (MO)AshokÎncă nu există evaluări
- Preblending of Raw Materia1Document26 paginiPreblending of Raw Materia1Mohammed Abdo100% (1)
- MikoritkDocument6 paginiMikoritkChris Jonathan Showip RouteÎncă nu există evaluări
- Activity Based Costing TestbanksDocument18 paginiActivity Based Costing TestbanksCharlene MinaÎncă nu există evaluări
- Aavi 3Document4 paginiAavi 3Arnie IldefonsoÎncă nu există evaluări
- Reflective Memo 1-PracticumDocument5 paginiReflective Memo 1-Practicumapi-400515862Încă nu există evaluări
- Financial Management of Public Sector Unit (PSU) - NotesDocument23 paginiFinancial Management of Public Sector Unit (PSU) - Notesbiz19100% (1)
- Voice Over Script For Pilot TestingDocument2 paginiVoice Over Script For Pilot TestingRichelle Anne Tecson ApitanÎncă nu există evaluări
- Dash8 200 300 Electrical PDFDocument35 paginiDash8 200 300 Electrical PDFCarina Ramo LakaÎncă nu există evaluări
- TRAVEL POLICY CARLO URRIZA OLIVAR Standard Insurance Co. Inc - Travel Protect - Print CertificateDocument4 paginiTRAVEL POLICY CARLO URRIZA OLIVAR Standard Insurance Co. Inc - Travel Protect - Print CertificateCarlo OlivarÎncă nu există evaluări
- Investing in Granada's Property Market - Gaspar LinoDocument1 paginăInvesting in Granada's Property Market - Gaspar LinoGaspar LinoÎncă nu există evaluări
- China's Military UAV Industry - 14 June 2013Document21 paginiChina's Military UAV Industry - 14 June 2013Deep Kanakia100% (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDe la EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedEvaluare: 5 din 5 stele5/5 (80)
- The Obesity Code: Unlocking the Secrets of Weight LossDe la EverandThe Obesity Code: Unlocking the Secrets of Weight LossEvaluare: 4 din 5 stele4/5 (6)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDe la EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDEvaluare: 5 din 5 stele5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeEvaluare: 2 din 5 stele2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe la EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityEvaluare: 4 din 5 stele4/5 (24)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDe la EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionEvaluare: 4 din 5 stele4/5 (404)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDe la EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisEvaluare: 4.5 din 5 stele4.5/5 (42)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDe la EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsEvaluare: 5 din 5 stele5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDe la EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDe la EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisEvaluare: 4 din 5 stele4/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDe la EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsÎncă nu există evaluări
- Why We Die: The New Science of Aging and the Quest for ImmortalityDe la EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityEvaluare: 4 din 5 stele4/5 (3)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDe la EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryEvaluare: 4 din 5 stele4/5 (44)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.De la EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Evaluare: 4.5 din 5 stele4.5/5 (110)
- Gut: the new and revised Sunday Times bestsellerDe la EverandGut: the new and revised Sunday Times bestsellerEvaluare: 4 din 5 stele4/5 (392)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisDe la EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisEvaluare: 3.5 din 5 stele3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDe la EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsEvaluare: 3.5 din 5 stele3.5/5 (3)
- The Marshmallow Test: Mastering Self-ControlDe la EverandThe Marshmallow Test: Mastering Self-ControlEvaluare: 4.5 din 5 stele4.5/5 (58)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingDe la EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingEvaluare: 4 din 5 stele4/5 (1138)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningDe la EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningEvaluare: 4 din 5 stele4/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDe la EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsEvaluare: 4.5 din 5 stele4.5/5 (169)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDe la EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessEvaluare: 4.5 din 5 stele4.5/5 (328)
- A Brief History of Intelligence: Evolution, AI, and the Five Breakthroughs That Made Our BrainsDe la EverandA Brief History of Intelligence: Evolution, AI, and the Five Breakthroughs That Made Our BrainsEvaluare: 4.5 din 5 stele4.5/5 (6)