S-ar putea să vă placă și
- Blood Pressure: Lying Sitting Standing Heart Rate: Rhythm: Respiratory Rate: Rhythm: Temperature: Weight: KG Bmi: kg/m2Document3 paginiBlood Pressure: Lying Sitting Standing Heart Rate: Rhythm: Respiratory Rate: Rhythm: Temperature: Weight: KG Bmi: kg/m2Analeah MalayaoÎncă nu există evaluări
- Assessment ToolDocument3 paginiAssessment ToolAnaleah MalayaoÎncă nu există evaluări
- Assessment ToolDocument3 paginiAssessment ToolAnaleah Malayao0% (1)
- Clinical Interview AdultDocument12 paginiClinical Interview AdultPrince Arora100% (1)
- Bipolar Check in PDFDocument2 paginiBipolar Check in PDFAnonymous 830d2u2UÎncă nu există evaluări
- Intake FormDocument8 paginiIntake FormYusra EjazÎncă nu există evaluări
- Guide Question Opd MomintsDocument6 paginiGuide Question Opd MomintsFaith Stephanie SantosÎncă nu există evaluări
- Assessment For Duty 2Document19 paginiAssessment For Duty 2Kim TangoÎncă nu există evaluări
- Mhi NPV PacketDocument10 paginiMhi NPV PacketCodyÎncă nu există evaluări
- MODULE 2 Developing The Whole PersonDocument29 paginiMODULE 2 Developing The Whole PersonJett Cabanatan NisolaÎncă nu există evaluări
- Medical History Taking FormDocument6 paginiMedical History Taking FormRoanne DivinagraciaÎncă nu există evaluări
- Health Assessment Form FINAL ProjectDocument10 paginiHealth Assessment Form FINAL ProjectClarence AbarratigueÎncă nu există evaluări
- General, Medical and Health Information: Lifestyle & Diabetes QuestionnaireDocument10 paginiGeneral, Medical and Health Information: Lifestyle & Diabetes QuestionnairerizkymutiaÎncă nu există evaluări
- Jbe Areas of Wellness - ResearchDocument8 paginiJbe Areas of Wellness - Researchapi-537847223Încă nu există evaluări
- Client Comprehensive Therapy Intake Form: Today's DateDocument8 paginiClient Comprehensive Therapy Intake Form: Today's DateLaura MichelÎncă nu există evaluări
- SLMC Returning Patient FemaleDocument2 paginiSLMC Returning Patient FemaleCatie Tan ChingÎncă nu există evaluări
- PD (Unit 1.2)Document25 paginiPD (Unit 1.2)Lyca de los SantosÎncă nu există evaluări
- Scala Calitate Viata PDFDocument3 paginiScala Calitate Viata PDFStefan SanduÎncă nu există evaluări
- Final Project PyschoDocument9 paginiFinal Project PyschoHannah PantilloÎncă nu există evaluări
- Emotional Wellness Checklist 2022 7Document2 paginiEmotional Wellness Checklist 2022 7Mourya S TejaÎncă nu există evaluări
- Gordon's Functional Health PatternDocument5 paginiGordon's Functional Health PatternBritney ApasÎncă nu există evaluări
- Ready Made Questions For GordonsDocument15 paginiReady Made Questions For GordonsKyl M. SrrcÎncă nu există evaluări
- Meaning of Life Workbook FINALDocument17 paginiMeaning of Life Workbook FINALSiva Kumar100% (1)
- 검진문진표 - Health Examination QuestionnaireDocument6 pagini검진문진표 - Health Examination QuestionnaireNabila Shaffa Rizky ChandraÎncă nu există evaluări
- For Parent/Guardian To CompleteDocument9 paginiFor Parent/Guardian To CompleteRhay NotorioÎncă nu există evaluări
- Choosing Sleep: An Acceptance and Commitment Therapy CourseDocument27 paginiChoosing Sleep: An Acceptance and Commitment Therapy CourseKitty G K'nkoÎncă nu există evaluări
- Emotional Wellness Checklist 2021 2Document2 paginiEmotional Wellness Checklist 2021 2Pooja SÎncă nu există evaluări
- Activities For Validating Feelings and Normalizing Reactions Activity 1 Name: Grade and SectionDocument11 paginiActivities For Validating Feelings and Normalizing Reactions Activity 1 Name: Grade and SectionHazel Ann SobrepeñaÎncă nu există evaluări
- General, Medical and Health Information: Lifestyle & Pre-Diabetes QuestionnaireDocument8 paginiGeneral, Medical and Health Information: Lifestyle & Pre-Diabetes QuestionnaireAndrei StefanÎncă nu există evaluări
- Adult and Adolescent Intake InterviewDocument5 paginiAdult and Adolescent Intake InterviewAidan AlexisÎncă nu există evaluări
- Stress ManagementDocument5 paginiStress Managementprashantmis452Încă nu există evaluări
- ActivitiesDocument34 paginiActivitiesHanna100% (2)
- JMDT 2 023 Figure 1 PDFDocument5 paginiJMDT 2 023 Figure 1 PDFMuhammadAL-AyubiÎncă nu există evaluări
- What'S Your Personality Type and Emotional Iq?: Ms. Estrella A. Pabecca, RGCDocument24 paginiWhat'S Your Personality Type and Emotional Iq?: Ms. Estrella A. Pabecca, RGCKidrock TupasÎncă nu există evaluări
- Introduction From Nancy Lonsdorf M.D.: Maharishi Vedic MedicineDocument81 paginiIntroduction From Nancy Lonsdorf M.D.: Maharishi Vedic Medicines muraÎncă nu există evaluări
- Anamnesis Psicológica (C)Document9 paginiAnamnesis Psicológica (C)rosaÎncă nu există evaluări
- Social Anxiety Screening ToolDocument5 paginiSocial Anxiety Screening ToolKurt CutayÎncă nu există evaluări
- Group-3-12-Respect-Standardized-Questionnaires EditedDocument5 paginiGroup-3-12-Respect-Standardized-Questionnaires EditedJoselle Cayanan LawÎncă nu există evaluări
- Taking My Vitamins: Nutritional MetabolicDocument5 paginiTaking My Vitamins: Nutritional MetabolicRichie VilaÎncă nu există evaluări
- Adult Case HistoryDocument16 paginiAdult Case HistoryLaiba AttiqueÎncă nu există evaluări
- Sleep CodebookDocument6 paginiSleep CodebookJunn Ree Montilla100% (1)
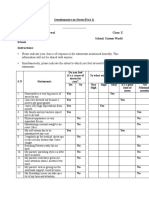
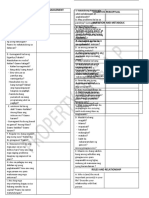
- Questionnaire On Stress - Part 1Document2 paginiQuestionnaire On Stress - Part 1khushi agarwalÎncă nu există evaluări
- Crisis Intervention ProformaDocument6 paginiCrisis Intervention Proformamathan kÎncă nu există evaluări
- Client Health Information (Psycle)Document8 paginiClient Health Information (Psycle)Suga's baeÎncă nu există evaluări
- Gordons 11 Functional Health PatternsDocument2 paginiGordons 11 Functional Health PatternsCathryn luv QuisidoÎncă nu există evaluări
- New Client Forms - Personal TrainingDocument44 paginiNew Client Forms - Personal Trainingalanna.snowden3Încă nu există evaluări
- Stress Management WorkshopDocument36 paginiStress Management WorkshopKim Layda BillonesÎncă nu există evaluări
- Assignment Topic Mental HealthDocument8 paginiAssignment Topic Mental HealthAsma SirajÎncă nu există evaluări
- Mental Health Awareness For WomenDocument55 paginiMental Health Awareness For WomenVanessa Devota Veloso - RamirezÎncă nu există evaluări
- Daily Lesson Plan StressDocument5 paginiDaily Lesson Plan StressRobert Andrew BaldadoÎncă nu există evaluări
- Quarter 2 Week 4-Day 4Document14 paginiQuarter 2 Week 4-Day 4Sen. Claro M. Recto Memorial Integrated School (Region IV-A - Lipa City)Încă nu există evaluări
- Clinical Assessment Questionnare 1Document13 paginiClinical Assessment Questionnare 1Iris FuedanÎncă nu există evaluări
- Modul EnglishDocument14 paginiModul EnglishNrhildaÎncă nu există evaluări
- Parent Intake InterviewDocument5 paginiParent Intake InterviewamandaÎncă nu există evaluări
- Stress LectureDocument2 paginiStress LectureRupelma PatnugotÎncă nu există evaluări
- New Questions 1Document2 paginiNew Questions 1ShobhitÎncă nu există evaluări
- Health Triangle Activity PacketDocument4 paginiHealth Triangle Activity Packetgustavo.martinezramirezÎncă nu există evaluări
- Gordons Helth PatternDocument6 paginiGordons Helth Pattern2000482Încă nu există evaluări
- Gordon's PrintableDocument2 paginiGordon's PrintableEmeEmekaÎncă nu există evaluări
- Pharma Finals 19Document12 paginiPharma Finals 19Mark Jheran Alvarez100% (1)
- College of Nursing Prelim Examination Pharmacology 1 Semester, SY 2019-2020 September 7, 2019 General DirectionDocument12 paginiCollege of Nursing Prelim Examination Pharmacology 1 Semester, SY 2019-2020 September 7, 2019 General DirectionMark Jheran Alvarez100% (1)
- Midterm Pharma 19Document11 paginiMidterm Pharma 19Mark Jheran Alvarez100% (1)
- Drug StudyDocument4 paginiDrug StudyMark Jheran AlvarezÎncă nu există evaluări
- Philippine Women's University Taft Ave, Manila School of NursingDocument1 paginăPhilippine Women's University Taft Ave, Manila School of NursingMark Jheran AlvarezÎncă nu există evaluări
- Eteeap-College of Nursing Midterm Examination NCM 103 Health Education 1st Semester SY 2019-2020 September 2, 2019Document1 paginăEteeap-College of Nursing Midterm Examination NCM 103 Health Education 1st Semester SY 2019-2020 September 2, 2019Mark Jheran AlvarezÎncă nu există evaluări
- Case Study 1Document12 paginiCase Study 1Mark Jheran AlvarezÎncă nu există evaluări
- Basic and Applied ResearchDocument1 paginăBasic and Applied ResearchMark Jheran AlvarezÎncă nu există evaluări
- Journal Appraisal 1Document35 paginiJournal Appraisal 1Mark Jheran AlvarezÎncă nu există evaluări
- Nomination Form PDFDocument1 paginăNomination Form PDFMark Jheran AlvarezÎncă nu există evaluări
- Case Study RespiDocument3 paginiCase Study RespiMark Jheran AlvarezÎncă nu există evaluări
- Pharma Neuro 1 PDFDocument115 paginiPharma Neuro 1 PDFMark Jheran AlvarezÎncă nu există evaluări
- (MT-RES) Manuscript Evaluation ToolDocument5 pagini(MT-RES) Manuscript Evaluation ToolAisle Malibiran PalerÎncă nu există evaluări
- Defense Proposal Evaluation Tool Version 2Document1 paginăDefense Proposal Evaluation Tool Version 2Mark Jheran AlvarezÎncă nu există evaluări
- Prof. Mark Jheran Alvarez, USRN, MAN-MSDocument52 paginiProf. Mark Jheran Alvarez, USRN, MAN-MSMark Jheran AlvarezÎncă nu există evaluări
- SyllabusDocument2 paginiSyllabusMark Jheran AlvarezÎncă nu există evaluări
- Defense Proposal Evaluation Tool Version 2Document1 paginăDefense Proposal Evaluation Tool Version 2Mark Jheran AlvarezÎncă nu există evaluări
- Prof. Mark Jheran Alvarez, USRN, MAN-MSDocument52 paginiProf. Mark Jheran Alvarez, USRN, MAN-MSMark Jheran AlvarezÎncă nu există evaluări
- Prof. Mark Jheran Alvarez, USRN, MAN-MSDocument52 paginiProf. Mark Jheran Alvarez, USRN, MAN-MSMark Jheran AlvarezÎncă nu există evaluări
- Beach: at TheDocument18 paginiBeach: at TheNhu NguyenÎncă nu există evaluări
- Titi Corn Is A Kind of Food Ingredient Made From Corn Raw Materials Whose Manufacturing Process Uses ToolsDocument2 paginiTiti Corn Is A Kind of Food Ingredient Made From Corn Raw Materials Whose Manufacturing Process Uses Toolsnurwasilatun silaÎncă nu există evaluări
- Usc Graduate Coursework CertificationDocument7 paginiUsc Graduate Coursework Certificationpodajokityk2100% (2)
- Work Report Human ValuesDocument12 paginiWork Report Human ValuesTeen BodybuildingÎncă nu există evaluări
- Standard Prestasi English Tingkatan 1 - ChecklistDocument2 paginiStandard Prestasi English Tingkatan 1 - ChecklistBin Hoon GanÎncă nu există evaluări
- Body Parts Lesson Plan FinalDocument5 paginiBody Parts Lesson Plan FinalCristina Stepan0% (1)
- Techno India University, Kolkata: (B.Tech Civil Engineering)Document3 paginiTechno India University, Kolkata: (B.Tech Civil Engineering)HimanshuÎncă nu există evaluări
- Final Action Plan 2019-2020Document7 paginiFinal Action Plan 2019-2020Gregory ArcadeÎncă nu există evaluări
- WidaDocument20 paginiWidaapi-448096857Încă nu există evaluări
- Kirtan Thakkar Official ResumeDocument2 paginiKirtan Thakkar Official Resumeapi-617398305Încă nu există evaluări
- Fm-Ro-19-01 - Request To CompleteDocument1 paginăFm-Ro-19-01 - Request To CompleteJericho MaganaÎncă nu există evaluări
- Week 5 FlowchartDocument1 paginăWeek 5 FlowchartAlexÎncă nu există evaluări
- Acog Embarazo Gemelar 2004 PDFDocument15 paginiAcog Embarazo Gemelar 2004 PDFEliel MarcanoÎncă nu există evaluări
- Aspen Posting Grades mp1Document10 paginiAspen Posting Grades mp1api-346876984Încă nu există evaluări
- Accommodative Insufficiency A Literature and Record ReviewDocument6 paginiAccommodative Insufficiency A Literature and Record ReviewPierre A. RodulfoÎncă nu există evaluări
- Fce Practice TestsDocument3 paginiFce Practice Testsjmaurp100% (1)
- Article 2: Releasing Your KarmaDocument2 paginiArticle 2: Releasing Your KarmaMOHAMMED MOUNIRÎncă nu există evaluări
- Boy Scout Coordinators' Level of Participation in Scouting and Its Impact On Their Self-Esteem and Job SatisfactionDocument9 paginiBoy Scout Coordinators' Level of Participation in Scouting and Its Impact On Their Self-Esteem and Job SatisfactionPsychology and Education: A Multidisciplinary JournalÎncă nu există evaluări
- Penilaian Preceptorship (Mini-Cex, Dops, Longcase, Soca) 2020Document49 paginiPenilaian Preceptorship (Mini-Cex, Dops, Longcase, Soca) 2020Dian tri febrianaÎncă nu există evaluări
- New Erf - Fy 2024 (Teacher Ii - Iii)Document4 paginiNew Erf - Fy 2024 (Teacher Ii - Iii)Sibs Academic ServicesÎncă nu există evaluări
- Chelline Dingal ResumeDocument1 paginăChelline Dingal ResumeLuffy KunÎncă nu există evaluări
- Physical Fitness in Physiotherapy Students Using Modified Harvard Step Test - A Pilot StudyDocument4 paginiPhysical Fitness in Physiotherapy Students Using Modified Harvard Step Test - A Pilot Studybistnu rachsÎncă nu există evaluări
- Postgraduate Prospectus 2021: World ChangersDocument35 paginiPostgraduate Prospectus 2021: World ChangersSKÎncă nu există evaluări
- Individual Assignment - LAN Proposal ITT459Document5 paginiIndividual Assignment - LAN Proposal ITT459Fahim Amar0% (1)
- Habitat Lesson-WetlandsDocument8 paginiHabitat Lesson-Wetlandsapi-270058879Încă nu există evaluări
- Patient Care Session 8 Flipped ClassroomDocument7 paginiPatient Care Session 8 Flipped ClassroomNurliyana Zairul AfendiÎncă nu există evaluări
- Foreign Service Officer Test (FSOT) Study GuideDocument20 paginiForeign Service Officer Test (FSOT) Study GuideMcRee Learning Center100% (1)
- Microglia in Alzhimers JCI PaperDocument11 paginiMicroglia in Alzhimers JCI PaperRavinder SinghÎncă nu există evaluări
- New Trends in Multicultural EducationDocument2 paginiNew Trends in Multicultural EducationFeyza EmillaÎncă nu există evaluări
- Final Udm Standard Syllabus - Social Work DocumentationDocument13 paginiFinal Udm Standard Syllabus - Social Work DocumentationBenneth DasoÎncă nu există evaluări
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe la EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityEvaluare: 4 din 5 stele4/5 (28)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDe la EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsEvaluare: 5 din 5 stele5/5 (1)
- Maktub: An Inspirational Companion to The AlchemistDe la EverandMaktub: An Inspirational Companion to The AlchemistEvaluare: 4.5 din 5 stele4.5/5 (3)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDe la EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsÎncă nu există evaluări
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeEvaluare: 2 din 5 stele2/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDe la EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDEvaluare: 5 din 5 stele5/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDe la EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionEvaluare: 4 din 5 stele4/5 (404)
- The Freedom of Self-Forgetfulness: The Path to True Christian JoyDe la EverandThe Freedom of Self-Forgetfulness: The Path to True Christian JoyEvaluare: 5 din 5 stele5/5 (192)
- No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems ModelDe la EverandNo Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems ModelEvaluare: 5 din 5 stele5/5 (4)
- Summary of The 48 Laws of Power: by Robert GreeneDe la EverandSummary of The 48 Laws of Power: by Robert GreeneEvaluare: 4.5 din 5 stele4.5/5 (233)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDe la EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedEvaluare: 5 din 5 stele5/5 (81)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDe la EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityEvaluare: 4 din 5 stele4/5 (3)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)De la EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Încă nu există evaluări
- Master Your Emotions: Develop Emotional Intelligence and Discover the Essential Rules of When and How to Control Your FeelingsDe la EverandMaster Your Emotions: Develop Emotional Intelligence and Discover the Essential Rules of When and How to Control Your FeelingsEvaluare: 4.5 din 5 stele4.5/5 (321)
- Codependent No More: How to Stop Controlling Others and Start Caring for YourselfDe la EverandCodependent No More: How to Stop Controlling Others and Start Caring for YourselfEvaluare: 5 din 5 stele5/5 (88)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDe la EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Pivot Year: 365 Days To Become The Person You Truly Want To BeDe la EverandThe Pivot Year: 365 Days To Become The Person You Truly Want To BeEvaluare: 4.5 din 5 stele4.5/5 (15)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDe la EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsEvaluare: 3.5 din 5 stele3.5/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.De la EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Evaluare: 4.5 din 5 stele4.5/5 (110)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisDe la EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisEvaluare: 3.5 din 5 stele3.5/5 (2)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDe la EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessEvaluare: 4.5 din 5 stele4.5/5 (328)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDe la EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeEvaluare: 4.5 din 5 stele4.5/5 (253)