S-ar putea să vă placă și
- 68th AACC Annual Scientific Meeting Abstract eBookDe la Everand68th AACC Annual Scientific Meeting Abstract eBookÎncă nu există evaluări
- New Microsoft Word DocumentDocument7 paginiNew Microsoft Word DocumentDocAxi Maximo Jr AxibalÎncă nu există evaluări
- CLINICAL CHEMISTRY: Passbooks Study GuideDe la EverandCLINICAL CHEMISTRY: Passbooks Study GuideÎncă nu există evaluări
- Resolution of ABO Discrepancies: FALSE POSITIVE Means The Reaction Should Have Been NEGATIVE ButDocument4 paginiResolution of ABO Discrepancies: FALSE POSITIVE Means The Reaction Should Have Been NEGATIVE ButJasmine Montero-GaribayÎncă nu există evaluări
- Study Stack - Hematology Tests 3-4 Table ReviewDocument5 paginiStudy Stack - Hematology Tests 3-4 Table Review장주연Încă nu există evaluări
- Study Stack - ASCP Coag Hematology Table ReviewDocument2 paginiStudy Stack - ASCP Coag Hematology Table Review장주연100% (1)
- Blood Banking: RH Blood Group SystemDocument2 paginiBlood Banking: RH Blood Group SystemRomie Solacito100% (1)
- Blood Bank2Document85 paginiBlood Bank22131443Încă nu există evaluări
- Incorrectly: CorrectlyDocument25 paginiIncorrectly: CorrectlypikachuÎncă nu există evaluări
- 2210 ABO Worksheet-1Document3 pagini2210 ABO Worksheet-1Lida LindstromÎncă nu există evaluări
- (CC) Case Study 1 and 2Document11 pagini(CC) Case Study 1 and 2Alyssa Nicole BarrettoÎncă nu există evaluări
- Lab Policies Complete Blood Count of Whole Blood On The Sysmex KX 21N - RB Lab 1535Document20 paginiLab Policies Complete Blood Count of Whole Blood On The Sysmex KX 21N - RB Lab 1535tomÎncă nu există evaluări
- Must To Know Is PDFDocument19 paginiMust To Know Is PDFKaycee Gretz LorescaÎncă nu există evaluări
- GeneralDocument31 paginiGeneralpikachu100% (1)
- Other Blood Group SystemsDocument2 paginiOther Blood Group SystemsRachel ManaloÎncă nu există evaluări
- Clinical ChemistryDocument7 paginiClinical ChemistryDale SuanoÎncă nu există evaluări
- Ascpi Recalls 1Document10 paginiAscpi Recalls 1Ben SabladaÎncă nu există evaluări
- ImmunohematologyDocument4 paginiImmunohematologyosama1381971Încă nu există evaluări
- Clinical Chemistry3Document81 paginiClinical Chemistry3Miguel Alfonso OlfatoÎncă nu există evaluări
- Board of Directors: Ascp-Ascp Certification & Qualification Comparison ChartDocument1 paginăBoard of Directors: Ascp-Ascp Certification & Qualification Comparison ChartMustaffah KabelyyonÎncă nu există evaluări
- ABO DiscrepanicesDocument12 paginiABO DiscrepanicesGlenn PerezÎncă nu există evaluări
- Blood Bank IDocument136 paginiBlood Bank IPerlie CÎncă nu există evaluări
- Clinical Chemistry IDocument8 paginiClinical Chemistry IMariel AbatayoÎncă nu există evaluări
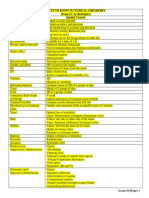
- MUST To KNOW in Clinical ChemistryDocument53 paginiMUST To KNOW in Clinical ChemistryTristan Jay CalabiaÎncă nu există evaluări
- Validation and Evaluation of Eight Commercially Available Point of Care CRP MethodsDocument7 paginiValidation and Evaluation of Eight Commercially Available Point of Care CRP MethodsAle AraujoÎncă nu există evaluări
- COMPLETE BLOOD COUNT Lecture GuideDocument9 paginiCOMPLETE BLOOD COUNT Lecture GuideKaycee Gretz LorescaÎncă nu există evaluări
- Blood BankDocument32 paginiBlood Bankpikachu100% (1)
- ABO Discrepancy Assignment Spring 2021Document5 paginiABO Discrepancy Assignment Spring 2021Ciarra AsuncionÎncă nu există evaluări
- Resolution of Abo DiscrepanciesDocument4 paginiResolution of Abo DiscrepanciesPatrick MabugatÎncă nu există evaluări
- Umbana Maria Christma Case Study - ProteinDocument3 paginiUmbana Maria Christma Case Study - ProteinGrace Umbaña YangaÎncă nu există evaluări
- BOC Study Guide: The MostDocument17 paginiBOC Study Guide: The MostDeanne LambanÎncă nu există evaluări
- Assessment and Management of Patients With Hematologic DisordersDocument20 paginiAssessment and Management of Patients With Hematologic Disorderschristine mercado100% (1)
- 3 Chemical Examination of UrineDocument82 pagini3 Chemical Examination of UrineJake Real Dela RocaÎncă nu există evaluări
- Blood Banking Chapter 1Document9 paginiBlood Banking Chapter 1throwawyÎncă nu există evaluări
- Adverse Reaction Blood BankDocument10 paginiAdverse Reaction Blood BankyourfamilydoctorÎncă nu există evaluări
- Medically Important VirusesDocument3 paginiMedically Important Virusesgiannpee100% (1)
- 2021 NEQAS-CC End-Cycle Webinar-Workshop Participant's Guide (August 12, 2022)Document5 pagini2021 NEQAS-CC End-Cycle Webinar-Workshop Participant's Guide (August 12, 2022)Chester KyleÎncă nu există evaluări
- Study Stacks - Chemistry Table Review PDFDocument14 paginiStudy Stacks - Chemistry Table Review PDF장주연100% (1)
- ENZYMOLOGYDocument2 paginiENZYMOLOGYCarla Lagar FloresÎncă nu există evaluări
- B Blab 7 Panel Spring 2012Document16 paginiB Blab 7 Panel Spring 2012pzaballero7063Încă nu există evaluări
- CLS Internship ManualDocument216 paginiCLS Internship ManualtaghamdÎncă nu există evaluări
- Blood Banking - Component PreparationDocument34 paginiBlood Banking - Component PreparationLentoOt EksDiiÎncă nu există evaluări
- Recall 1Document4 paginiRecall 1pikachuÎncă nu există evaluări
- Coagulation NotesDocument14 paginiCoagulation NotesthrowawyÎncă nu există evaluări
- Lesson 5: Nature of The Clinical LaboratoryDocument8 paginiLesson 5: Nature of The Clinical LaboratoryJohn Daniel AriasÎncă nu există evaluări
- IMH100 2nd Handout - Immunology Part II and ABO Blood GroupDocument4 paginiIMH100 2nd Handout - Immunology Part II and ABO Blood GroupnicholeÎncă nu există evaluări
- Detection of AntibodiesDocument7 paginiDetection of AntibodiesJezreeljeanne Largo CaparosoÎncă nu există evaluări
- Mega Micro para Table 1 (1) (PDF - Io)Document81 paginiMega Micro para Table 1 (1) (PDF - Io)CheryldaneBaculiÎncă nu există evaluări
- Blood Bank 4 DiscpDocument20 paginiBlood Bank 4 DiscpHector de la CruzÎncă nu există evaluări
- HemaDocument59 paginiHemaSteph VeeÎncă nu există evaluări
- Antibody IdentificationDocument27 paginiAntibody Identificationhamaada100% (1)
- Abo Typing Discrepancies: Rene Jesus Alfredo R. Dinglasan, RMTDocument14 paginiAbo Typing Discrepancies: Rene Jesus Alfredo R. Dinglasan, RMTdirenjan100% (1)
- Streptococcus, Entrococcus and Other Catalayse Negative GramDocument15 paginiStreptococcus, Entrococcus and Other Catalayse Negative GramKeen ManalastasÎncă nu există evaluări
- Chapter Blood: RBC Platelet HemostasisDocument89 paginiChapter Blood: RBC Platelet Hemostasisapi-19916399100% (1)
- Blood Bank TypingDocument34 paginiBlood Bank TypingSkylarÎncă nu există evaluări
- ML7111 MCQs Answers March 2020Document15 paginiML7111 MCQs Answers March 2020Cleo SalvadorÎncă nu există evaluări
- ML7111 MCQs Answers April 2020Document16 paginiML7111 MCQs Answers April 2020Cleo SalvadorÎncă nu există evaluări
- Quick Review Cards For Medical Laboratory Science - Polansky, Valerie DietzDocument619 paginiQuick Review Cards For Medical Laboratory Science - Polansky, Valerie DietzIslam92% (86)
- Yacon Lyophilization LetterDocument1 paginăYacon Lyophilization LetterJayrone James FuerteÎncă nu există evaluări
- Hydrolysis of StarchDocument5 paginiHydrolysis of StarchJayrone James FuerteÎncă nu există evaluări
- Supplementary Information Sheet (1) - 2Document1 paginăSupplementary Information Sheet (1) - 2Jayrone James FuerteÎncă nu există evaluări
- Example #1: 53.4 ML of A 1.50 M Solution of Nacl Is On Hand, But You Need SomeDocument4 paginiExample #1: 53.4 ML of A 1.50 M Solution of Nacl Is On Hand, But You Need SomeJayrone James FuerteÎncă nu există evaluări
- FCL 1Document3 paginiFCL 1Jayrone James FuerteÎncă nu există evaluări
- Biology Vocabulary GlossaryDocument14 paginiBiology Vocabulary GlossaryElijah CastroÎncă nu există evaluări
- Pharmaceutical BotanyDocument10 paginiPharmaceutical BotanyJan Chrispian MirasolÎncă nu există evaluări
- BioinformaticsDocument167 paginiBioinformaticsGilbert MethewÎncă nu există evaluări
- Nitrobacter WinogradskyDocument7 paginiNitrobacter WinogradskyFerryKurniawanÎncă nu există evaluări
- Fifth Edition Answers To End-Of-Chapter Questions: GCSE Biology For YouDocument1 paginăFifth Edition Answers To End-Of-Chapter Questions: GCSE Biology For YouclydeÎncă nu există evaluări
- 7 week:: Microbial Growth (미생물의 성장)Document24 pagini7 week:: Microbial Growth (미생물의 성장)MoonHoLeeÎncă nu există evaluări
- Concepts of BiologyDocument1.007 paginiConcepts of BiologyEduardo Panadero CuarteroÎncă nu există evaluări
- Natural Antimicrobial and Bioactive Compounds From Ludwigia Parviflora RoxbDocument6 paginiNatural Antimicrobial and Bioactive Compounds From Ludwigia Parviflora Roxbnguyen ba trungÎncă nu există evaluări
- Classifying Living ThingsDocument8 paginiClassifying Living Thingsdesco2011Încă nu există evaluări
- General Zoology Module 1 Arthropoda and EchinodermataDocument5 paginiGeneral Zoology Module 1 Arthropoda and EchinodermataPaul PanizaÎncă nu există evaluări
- Laboratory Manual and GuidelineDocument27 paginiLaboratory Manual and GuidelineFatih Rushdi100% (1)
- Human Biology 12th Edition Test Bank Sylvia MaderDocument41 paginiHuman Biology 12th Edition Test Bank Sylvia MaderPaul Tilghman100% (28)
- 1 Plant PhysiologyDocument11 pagini1 Plant PhysiologyAidana MissÎncă nu există evaluări
- Superoxide Dismutase (SOD) A Promising Enzyme in The Area of Biopharmaceuticals in Its Native and Immobilized Form A ReviewDocument9 paginiSuperoxide Dismutase (SOD) A Promising Enzyme in The Area of Biopharmaceuticals in Its Native and Immobilized Form A ReviewIJRASETPublicationsÎncă nu există evaluări
- Evolution The History of An Idea Bowler PDFDocument2 paginiEvolution The History of An Idea Bowler PDFJessica0% (4)
- Dermo Disease of OysterDocument4 paginiDermo Disease of OysterSophia ManzanoÎncă nu există evaluări
- Biology Practical Class 12Document2 paginiBiology Practical Class 12ManishÎncă nu există evaluări
- Science August 14 2009Document95 paginiScience August 14 2009Greg_G100% (1)
- Tips For BiologyDocument15 paginiTips For BiologyMasega Daniel ManaliÎncă nu există evaluări
- The Digestive SystemDocument2 paginiThe Digestive SystemAutumn GarofolaÎncă nu există evaluări
- Report PDFDocument6 paginiReport PDFAayushiÎncă nu există evaluări
- The Five Kingdom Classification System ArticleDocument3 paginiThe Five Kingdom Classification System ArticleNermine AbedÎncă nu există evaluări
- EBMT 2021 ProgramDocument288 paginiEBMT 2021 Programtirillas101Încă nu există evaluări
- Transgene: Transparent FrogDocument3 paginiTransgene: Transparent Froggeobee emmanuelÎncă nu există evaluări
- Gene MappingDocument5 paginiGene MappingC/fataax C/xakiimÎncă nu există evaluări
- Zhao Et Al 2021 Pentatoma Rufipes MitogenomeDocument22 paginiZhao Et Al 2021 Pentatoma Rufipes MitogenomeDávid RédeiÎncă nu există evaluări
- 1ST SA BIOCHEMISTRY - AlmendrasDocument5 pagini1ST SA BIOCHEMISTRY - AlmendrasCherry DagohoyÎncă nu există evaluări
- Human Biology 12th Edition Test Bank Sylvia MaderDocument41 paginiHuman Biology 12th Edition Test Bank Sylvia Maderdorislanhpr028Încă nu există evaluări
- Godbout, J. P., & Glaser, R. (2006) - Stress-Induced Immune Dysregulation. Implications For Wound Healing, Infectious Disease and CancerDocument7 paginiGodbout, J. P., & Glaser, R. (2006) - Stress-Induced Immune Dysregulation. Implications For Wound Healing, Infectious Disease and CancerFranco Paolo Maray-GhigliottoÎncă nu există evaluări
- Worksheet - Metabolism Seventh GradeDocument2 paginiWorksheet - Metabolism Seventh Gradeerika alzateÎncă nu există evaluări