S-ar putea să vă placă și
- ScriptDocument12 paginiScriptWaleed Nadeem50% (2)
- Pathophysiology SARSDocument4 paginiPathophysiology SARSStephanie Joy Escala71% (7)
- Counselling LetterDocument1 paginăCounselling LetterSeann LorescoÎncă nu există evaluări
- MannitolDocument3 paginiMannitolAlexandra AntondyÎncă nu există evaluări
- Drug StudyDocument5 paginiDrug StudyGAYOL BREEN IRAH A.Încă nu există evaluări
- Precipitating Factor Predisposing FactorsDocument1 paginăPrecipitating Factor Predisposing FactorsanthropusÎncă nu există evaluări
- Dental Prob NCPDocument3 paginiDental Prob NCPx483xDÎncă nu există evaluări
- NCP OsteosarcomaDocument6 paginiNCP OsteosarcomaNiksÎncă nu există evaluări
- Schematic Diagram BA HAP HRDocument2 paginiSchematic Diagram BA HAP HRMika MinsalanÎncă nu există evaluări
- 100QforCIP 30QforDiagnosticReviewDocument29 pagini100QforCIP 30QforDiagnosticReviewpamgelÎncă nu există evaluări
- Psych - Chapter 23 Into To Milieu ManagementDocument4 paginiPsych - Chapter 23 Into To Milieu ManagementKaren かれんÎncă nu există evaluări
- Nursing AssessmentDocument4 paginiNursing AssessmentFlor SabaysabayÎncă nu există evaluări
- Burn - Daily Physical AssessmentDocument8 paginiBurn - Daily Physical AssessmentkrishcelÎncă nu există evaluări
- SLE PathophysiologyDocument3 paginiSLE PathophysiologyyasiraÎncă nu există evaluări
- Nursing Care Plan: Acute Pain Related To Inflammatory Response Secondary To InfectionDocument2 paginiNursing Care Plan: Acute Pain Related To Inflammatory Response Secondary To InfectionTammy De GuzmanÎncă nu există evaluări
- Drug Study Domperidone CompressDocument1 paginăDrug Study Domperidone CompressAngelica TolledoÎncă nu există evaluări
- FINALS ReviewerDocument14 paginiFINALS ReviewerJustine Simeon lagunzadÎncă nu există evaluări
- PathophysiologyDocument9 paginiPathophysiologySuzette PipoÎncă nu există evaluări
- Name of Drug Dosage, Route, Frequency and Timing Mechanism of Action Indication Adverse Reactions Special Precautions Nursing ResponsibilitiesDocument2 paginiName of Drug Dosage, Route, Frequency and Timing Mechanism of Action Indication Adverse Reactions Special Precautions Nursing ResponsibilitiesIvan Matthew SuperioÎncă nu există evaluări
- Acute Pain NCPDocument2 paginiAcute Pain NCPfbarlicosÎncă nu există evaluări
- Running Head: Comprehensive Case Study 1Document11 paginiRunning Head: Comprehensive Case Study 1api-546355462Încă nu există evaluări
- Prioritization of Problems Health Problem:: Carlatan, San Fernando City, La UnionDocument4 paginiPrioritization of Problems Health Problem:: Carlatan, San Fernando City, La UnionGabrielle John HernaezÎncă nu există evaluări
- ASSESSMENTDocument2 paginiASSESSMENTColeen PequitÎncă nu există evaluări
- 51 100Document18 pagini51 100Jaessa Feliciano100% (1)
- Cefadroxil DuricefDocument1 paginăCefadroxil Duricefstaylor235Încă nu există evaluări
- HERNIADocument27 paginiHERNIAVanessa SumalbagÎncă nu există evaluări
- Huntingtons Disease NCPDocument4 paginiHuntingtons Disease NCPJerich Mark SalasÎncă nu există evaluări
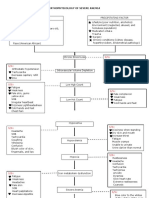
- Pathophysiology of Severe AnemiaDocument3 paginiPathophysiology of Severe AnemiaChrizley Shawn DeroniaÎncă nu există evaluări
- BARANDINO, Jia Laurice (Gouty Arthritis)Document18 paginiBARANDINO, Jia Laurice (Gouty Arthritis)Deinielle Magdangal RomeroÎncă nu există evaluări
- Psych NCPDocument4 paginiPsych NCPnoman-053Încă nu există evaluări
- AppendectomyDocument35 paginiAppendectomyleighjagÎncă nu există evaluări
- Surgical InstrumentDocument5 paginiSurgical Instrumentria_soriano_2100% (1)
- Pneumonia PathoDocument2 paginiPneumonia PathoDerick Nyl PascualÎncă nu există evaluări
- Electrical Burn PathophysiologyDocument1 paginăElectrical Burn PathophysiologydanicaÎncă nu există evaluări
- LFDDocument3 paginiLFDVhince Norben PiscoÎncă nu există evaluări
- Attapulgite PDFDocument1 paginăAttapulgite PDFWindy Tonapa100% (1)
- Pathophysiology, Bone CancerDocument7 paginiPathophysiology, Bone CancerMaria Grace Raquel Ormeneta100% (1)
- Movie Wit Scholarly AssignmentDocument10 paginiMovie Wit Scholarly Assignmentapi-283868512Încă nu există evaluări
- CiprobayDocument2 paginiCiprobayianecunar100% (1)
- Activity 6 - Drug StudyDocument14 paginiActivity 6 - Drug StudyAl-Mujib TanogÎncă nu există evaluări
- Pathophysiology of Pediculosis CapitisDocument1 paginăPathophysiology of Pediculosis CapitisAldrin Ian Oraza Alpe0% (1)
- Pathophysiology Cholelithiasis 2Document2 paginiPathophysiology Cholelithiasis 2Jamie HaravataÎncă nu există evaluări
- Drug Study EditedDocument5 paginiDrug Study EditedfabtaciousVeelaÎncă nu există evaluări
- PYOMYOSITISDocument6 paginiPYOMYOSITISChristine CoridoÎncă nu există evaluări
- Essay 1Document2 paginiEssay 1Geraldine ArellanoÎncă nu există evaluări
- Pathophysiology of Multiple Myeloma OkDocument3 paginiPathophysiology of Multiple Myeloma OkRifa'atul MahmudahÎncă nu există evaluări
- FNCP Final FinalDocument51 paginiFNCP Final FinalMichael Piduca100% (1)
- Self-Care Deficit Related To Inability To Perceive Body Part (Bathing)Document2 paginiSelf-Care Deficit Related To Inability To Perceive Body Part (Bathing)lilpeabea100% (1)
- MyelomeningoceleDocument7 paginiMyelomeningocelemavefigÎncă nu există evaluări
- Annotated Group 2 Impetigo Concept Mapping 1Document30 paginiAnnotated Group 2 Impetigo Concept Mapping 1DHANE ANN CAMPOSANOÎncă nu există evaluări
- Content: Outline Form Only Make A Separate Sheet For The Content. The Health Teaching Plan Should Focus On Home Care For Patients With Mood DisorderDocument4 paginiContent: Outline Form Only Make A Separate Sheet For The Content. The Health Teaching Plan Should Focus On Home Care For Patients With Mood DisorderRaffy Sebastian Seballos100% (1)
- (Brand Name) & Date Ordered General Class and Family Specific IndicationDocument2 pagini(Brand Name) & Date Ordered General Class and Family Specific IndicationNicole Grace VillegasÎncă nu există evaluări
- Nursing Care Plan: Subjective: During 8 Hours Nursing Management: (5) After 8 HoursDocument4 paginiNursing Care Plan: Subjective: During 8 Hours Nursing Management: (5) After 8 HoursRawan KhateebÎncă nu există evaluări
- Acute Gastroenteritis With Severe DehydrationDocument22 paginiAcute Gastroenteritis With Severe DehydrationCess Dunwan100% (1)
- Nursing Care Plan #1 Cues Nursing Diagnosis Objectives Intervention Rationale Evaluation Subjective: Short Term: Independent: Independent Short TermDocument5 paginiNursing Care Plan #1 Cues Nursing Diagnosis Objectives Intervention Rationale Evaluation Subjective: Short Term: Independent: Independent Short TermAlmer OstreaÎncă nu există evaluări
- CASE STUDY (Gastro)Document3 paginiCASE STUDY (Gastro)Jake Yvan DizonÎncă nu există evaluări
- Management of Tuberculosis: A guide for clinicians (eBook edition)De la EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Încă nu există evaluări
- Illustrator File Edit Select Effect View Window HelpDocument8 paginiIllustrator File Edit Select Effect View Window HelpHaizel BieberÎncă nu există evaluări
- Ear DisorderDocument61 paginiEar DisorderSakthi DeviÎncă nu există evaluări
- Sharp Int Market V CA +LBP & VistanDocument7 paginiSharp Int Market V CA +LBP & VistanJoe RealÎncă nu există evaluări
- Gaboya V CuiDocument11 paginiGaboya V CuiJoe RealÎncă nu există evaluări
- Title Vi - Usufruct Chapter One: Usufruct in General: Property NotesDocument16 paginiTitle Vi - Usufruct Chapter One: Usufruct in General: Property NotesJoe RealÎncă nu există evaluări
- People v. MadragaDocument2 paginiPeople v. MadragaJoe RealÎncă nu există evaluări
- Luz Farms V Sec of DarDocument9 paginiLuz Farms V Sec of DarJoe RealÎncă nu există evaluări
- American Wire and Cable Daily Rated Employees Union v. American Wire and CableDocument11 paginiAmerican Wire and Cable Daily Rated Employees Union v. American Wire and CableJoe RealÎncă nu există evaluări
- 3 (6) Baluran V NavarroDocument6 pagini3 (6) Baluran V NavarroJoe RealÎncă nu există evaluări
- Taglay v. Judge Trabajo Daray DigestDocument2 paginiTaglay v. Judge Trabajo Daray DigestJoe RealÎncă nu există evaluări
- Moralidad V Sps PernesDocument8 paginiMoralidad V Sps PernesJoe RealÎncă nu există evaluări
- Rivera-Calingasan V RiveraDocument8 paginiRivera-Calingasan V RiveraJoe RealÎncă nu există evaluări
- Pldt-vs-Arceo-digestDocument3 paginiPldt-vs-Arceo-digestJoe RealÎncă nu există evaluări
- First Division G.R. No. 193493, June 13, 2013: Supreme Court of The PhilippinesDocument15 paginiFirst Division G.R. No. 193493, June 13, 2013: Supreme Court of The PhilippinesJoe RealÎncă nu există evaluări
- Royal Plant Workers Union v. Coca Cola BottlersDocument5 paginiRoyal Plant Workers Union v. Coca Cola BottlersJoe RealÎncă nu există evaluări
- Asis v. Minister of LaborDocument4 paginiAsis v. Minister of LaborJoe RealÎncă nu există evaluări
- Poseidon Fishing v. NLRC, February 20, 2006Document14 paginiPoseidon Fishing v. NLRC, February 20, 2006Joe RealÎncă nu există evaluări
- Exodus International Construction v. Biscocho, February 23, 2011Document11 paginiExodus International Construction v. Biscocho, February 23, 2011Joe RealÎncă nu există evaluări
- 15 Nestle Philippines, Inc. v. Puedan, JR.Document4 pagini15 Nestle Philippines, Inc. v. Puedan, JR.Joe RealÎncă nu există evaluări
- 13 (10) Manila Memorial Park Cemetery v. LuizDocument3 pagini13 (10) Manila Memorial Park Cemetery v. LuizJoe RealÎncă nu există evaluări
- Mingoa V LRADocument4 paginiMingoa V LRAJoe RealÎncă nu există evaluări
- St. Mary's University v. CA, March 8, 2005Document6 paginiSt. Mary's University v. CA, March 8, 2005Joe RealÎncă nu există evaluări
- de La Salle University Araneta v. Bernardo, February 13, 2017Document17 paginide La Salle University Araneta v. Bernardo, February 13, 2017Joe RealÎncă nu există evaluări
- Case Digest LaborDocument2 paginiCase Digest LaborJoe RealÎncă nu există evaluări
- San Miguel Corporation Vs AballaDocument4 paginiSan Miguel Corporation Vs AballaJoe RealÎncă nu există evaluări
- 12 (19) Diamond Farms v. Farms Agrarian Reform Beneficiaries Multi-Purpose CooperativeDocument19 pagini12 (19) Diamond Farms v. Farms Agrarian Reform Beneficiaries Multi-Purpose CooperativeJoe RealÎncă nu există evaluări
- PAL v. Ligan (G.R. No. 146408) : Investment Which Relates To The Job, Work or Service To BeDocument3 paginiPAL v. Ligan (G.R. No. 146408) : Investment Which Relates To The Job, Work or Service To BeJoe RealÎncă nu există evaluări
- Meralco Industrial Engineering Services v. NLRCDocument5 paginiMeralco Industrial Engineering Services v. NLRCJoe RealÎncă nu există evaluări
- Pardell V BartolomeDocument1 paginăPardell V BartolomeJoe RealÎncă nu există evaluări
- Teng v. PahagacDocument13 paginiTeng v. PahagacJoe RealÎncă nu există evaluări
- Sales Case ListDocument6 paginiSales Case ListJoe RealÎncă nu există evaluări
- Florencio Ignao Vs IacDocument1 paginăFlorencio Ignao Vs IacJoe RealÎncă nu există evaluări
- 06.03.01 TBL Hearing Loss and TinnitusDocument11 pagini06.03.01 TBL Hearing Loss and TinnitusJeff AguilarÎncă nu există evaluări
- Otitis Externa Case StudyDocument5 paginiOtitis Externa Case StudyGino Al Ballano BorinagaÎncă nu există evaluări
- Identification and Antimicrobial Susceptibility Patterns of Bacteria Causing Otitis Externa in DogsDocument10 paginiIdentification and Antimicrobial Susceptibility Patterns of Bacteria Causing Otitis Externa in DogsFadhil ShalihÎncă nu există evaluări
- (APJ) Common ENT CasesDocument31 pagini(APJ) Common ENT CasesApryl Phyllis JimenezÎncă nu există evaluări
- Perichondritis: Shah Darshan, George LijiDocument4 paginiPerichondritis: Shah Darshan, George LijiThasia IsabelitaÎncă nu există evaluări
- Complete Small Med Surgery 2Document65 paginiComplete Small Med Surgery 2MelanieÎncă nu există evaluări
- Birao Sas 12 Microbiology and ParasitologyDocument8 paginiBirao Sas 12 Microbiology and ParasitologyFrancis Jacob Dejecacion GarcesÎncă nu există evaluări
- Otomycosis: Yan Edward, Dolly IrfandyDocument6 paginiOtomycosis: Yan Edward, Dolly IrfandyM Reza Kurnia AliÎncă nu există evaluări
- Otitis ExternaDocument19 paginiOtitis ExternaEren YooÎncă nu există evaluări
- Original Article: A Clinical and Microbial Study of Otomycosis: An Original StudyDocument9 paginiOriginal Article: A Clinical and Microbial Study of Otomycosis: An Original StudywennyrhyÎncă nu există evaluări
- Burton's Microbiology For The Health Sciences: Chapter 19. Bacterial InfectionsDocument29 paginiBurton's Microbiology For The Health Sciences: Chapter 19. Bacterial Infectionsmirai desuÎncă nu există evaluări
- Common ENT Conditions PwPT2008Document75 paginiCommon ENT Conditions PwPT2008Garlic BreadÎncă nu există evaluări
- Special Organs-Eye, Ear, NoseDocument15 paginiSpecial Organs-Eye, Ear, Noseعبدالسلام الأسمرÎncă nu există evaluări
- Neurology and Special Senses ' Neurology and Special Senses ' Section IiiDocument20 paginiNeurology and Special Senses ' Neurology and Special Senses ' Section IiiLuis Jose VelazquezÎncă nu există evaluări
- HEALTH 6 W2 D1 Personal Health IssuesDocument25 paginiHEALTH 6 W2 D1 Personal Health IssuesArenas JenÎncă nu există evaluări
- Chapter 50 Vision and HearingDocument7 paginiChapter 50 Vision and HearingAlmer OstreaÎncă nu există evaluări
- Ent-Book2 009 PDFDocument186 paginiEnt-Book2 009 PDFMariana Salgar100% (1)
- 1st Summative Test in MAPEH 6 1st QuarterDocument3 pagini1st Summative Test in MAPEH 6 1st QuarterArenas Jen100% (5)
- PLAB1 Quick Revision Al-Khair Water MarkedDocument337 paginiPLAB1 Quick Revision Al-Khair Water MarkedAhmed Bekhet100% (1)
- CR JiwDocument4 paginiCR JiwRizky Bayu AjieÎncă nu există evaluări
- Secundum Artem: Compounding For Otic DisordersDocument0 paginiSecundum Artem: Compounding For Otic Disordersdebieyolanda_7180456Încă nu există evaluări
- Fungal Otitis Externa As A Cause of Tympanic Membrane Perforation: A Case SeriesDocument6 paginiFungal Otitis Externa As A Cause of Tympanic Membrane Perforation: A Case Serieszerin_atinÎncă nu există evaluări
- Neha ShahDocument448 paginiNeha ShahAshima GautamÎncă nu există evaluări
- Health 6 Q1 Mod1 Lesson1 Personal-Health-Issues-And-Concerns v2Document23 paginiHealth 6 Q1 Mod1 Lesson1 Personal-Health-Issues-And-Concerns v2Gessle GamirÎncă nu există evaluări
- Otitis Externa Swimmers EarDocument2 paginiOtitis Externa Swimmers EarMilanisti22Încă nu există evaluări
- PI Otocomb OticDocument6 paginiPI Otocomb Oticdebieyolanda_7180456Încă nu există evaluări
- (CR) Chronic Otomycosis Due To Malassezia SPPDocument3 pagini(CR) Chronic Otomycosis Due To Malassezia SPPHendra SusantoÎncă nu există evaluări
- Ear, Nose, and Throat EmergenciesDocument23 paginiEar, Nose, and Throat EmergenciesRajesh SharmaÎncă nu există evaluări
- EnT - 1.01 External Ear (Dr. Opulencia)Document11 paginiEnT - 1.01 External Ear (Dr. Opulencia)jessicaeliseÎncă nu există evaluări
- NR 509 Final Exam Review-2Document50 paginiNR 509 Final Exam Review-2Lou EscobarÎncă nu există evaluări