S-ar putea să vă placă și
- Overview of Skin Aging and PhotoagingDocument7 paginiOverview of Skin Aging and PhotoagingtissanÎncă nu există evaluări
- Poly L Lactic Acid SicklesDocument4 paginiPoly L Lactic Acid SicklesRafael Autran Cavalcante AraújoÎncă nu există evaluări
- Minimally Invasive Face-Lifting: S-Lift and S-Plus Lift RhytidectomiesDocument11 paginiMinimally Invasive Face-Lifting: S-Lift and S-Plus Lift RhytidectomiesAditi SharmaÎncă nu există evaluări
- 311 PDFDocument10 pagini311 PDFFerry CahyadiÎncă nu există evaluări
- Mandelic Acid Chemical Peel in Acne Vulgaris: A Boon or A Bane?Document4 paginiMandelic Acid Chemical Peel in Acne Vulgaris: A Boon or A Bane?IOSRjournalÎncă nu există evaluări
- Lip Augmentation Using 4mm NeedleDocument3 paginiLip Augmentation Using 4mm NeedleNathaliaÎncă nu există evaluări
- Dermatrix - Radiofrequency Facial Rejuvenation Evidence-Based Effect IraildesDocument12 paginiDermatrix - Radiofrequency Facial Rejuvenation Evidence-Based Effect IraildesTatiane MouraÎncă nu există evaluări
- Soft Tissue Augmentation With Dermal Fillers, Part 1: Lips and Lower FaceDocument6 paginiSoft Tissue Augmentation With Dermal Fillers, Part 1: Lips and Lower FaceMichele CarvalhoÎncă nu există evaluări
- Collagen StimulatorsDocument11 paginiCollagen StimulatorsElizabeth TovittoÎncă nu există evaluări
- Novel Liposuction Techniques For The Treatment of HIV-Associated Dorsocervical Fat Pad and Parotid HypertrophyDocument15 paginiNovel Liposuction Techniques For The Treatment of HIV-Associated Dorsocervical Fat Pad and Parotid HypertrophyAng BiÎncă nu există evaluări
- AntiAging TherapiesDocument4 paginiAntiAging TherapiesRavvaÎncă nu există evaluări
- Basics of Dermal Filler Rheology.2Document7 paginiBasics of Dermal Filler Rheology.2Imanuel CristiantoÎncă nu există evaluări
- Lower Blepharoplasty: How To Avoid Complications: Dr. Vincent KH KWANDocument3 paginiLower Blepharoplasty: How To Avoid Complications: Dr. Vincent KH KWANHadi FirmansyahÎncă nu există evaluări
- Fitzpatric ScaleDocument4 paginiFitzpatric ScaleGligorpaulaÎncă nu există evaluări
- 2014 Stabilized Hyaluronic Acid Gel For Volume Restoration and Contouring of The ButtocksDocument9 pagini2014 Stabilized Hyaluronic Acid Gel For Volume Restoration and Contouring of The ButtocksMichele CarvalhoÎncă nu există evaluări
- Botulinum Toxin in Aesthetic Medicine Myths and RealitiesDocument12 paginiBotulinum Toxin in Aesthetic Medicine Myths and RealitiesЩербакова ЛенаÎncă nu există evaluări
- LL ALLUZIENCE Liquid Formulation of AbobotulinumtoxinA A 6-MonthDocument13 paginiLL ALLUZIENCE Liquid Formulation of AbobotulinumtoxinA A 6-MonthAnderson GomesÎncă nu există evaluări
- ACE Group Patient Leaflet Dermal FillersDocument9 paginiACE Group Patient Leaflet Dermal FillersJim MackieÎncă nu există evaluări
- Use of Lasers IPL 1Document86 paginiUse of Lasers IPL 1pippo07Încă nu există evaluări
- Alopecia Androgenética.. Uma Atualização Das Opções de Tratamento (Traduzir Artigo)Document16 paginiAlopecia Androgenética.. Uma Atualização Das Opções de Tratamento (Traduzir Artigo)Alexia Vieira de SouzaÎncă nu există evaluări
- Sculptra - Artigo PDFDocument3 paginiSculptra - Artigo PDFjulianaÎncă nu există evaluări
- Natox - Natural FaceliftDocument2 paginiNatox - Natural FaceliftLiliana LesuÎncă nu există evaluări
- Tear Trough LigamentDocument11 paginiTear Trough LigamentSuc Khoe la VangÎncă nu există evaluări
- Emerging Trends in Botulinum Neurotoxin A Resistance - An International Multidisciplinary Review and Consensus - Ho, 2022Document11 paginiEmerging Trends in Botulinum Neurotoxin A Resistance - An International Multidisciplinary Review and Consensus - Ho, 2022Rafael Autran Cavalcante AraújoÎncă nu există evaluări
- Hyaluron Pens: I Have A Question!Document3 paginiHyaluron Pens: I Have A Question!Xama CortijoÎncă nu există evaluări
- Update On The Management of Keloids: A. Paul Kelly, MDDocument6 paginiUpdate On The Management of Keloids: A. Paul Kelly, MDBudi KusumaÎncă nu există evaluări
- Step by Step Chemical Peels (Niti Khunger) (Z-Library)Document357 paginiStep by Step Chemical Peels (Niti Khunger) (Z-Library)viras1216Încă nu există evaluări
- Mesoglow y MesoliftDocument2 paginiMesoglow y MesoliftPablo BaudinoÎncă nu există evaluări
- Niumee Price List 2018Document26 paginiNiumee Price List 2018Anonymous XiZx8SbQBÎncă nu există evaluări
- Epidermal Growth Factor in Aesthetics and Regenerative Medicine Systematic ReviewDocument10 paginiEpidermal Growth Factor in Aesthetics and Regenerative Medicine Systematic ReviewDubraska SuárezÎncă nu există evaluări
- Informed Consent - Chemical Skin Peels and Treatments 2016Document10 paginiInformed Consent - Chemical Skin Peels and Treatments 2016Ashraf AboÎncă nu există evaluări
- Hugues Cartier, MD, Per Hed En, MD, Henry Delmar, MD, Per Bergentz, MD, Cecilia Skoglund, PHD, Carolina Edwartz, PHD, Maria Norberg, PHD, and Philippe Kestemont, MDDocument11 paginiHugues Cartier, MD, Per Hed En, MD, Henry Delmar, MD, Per Bergentz, MD, Cecilia Skoglund, PHD, Carolina Edwartz, PHD, Maria Norberg, PHD, and Philippe Kestemont, MDfake87734Încă nu există evaluări
- "No-Touch" Technique For Lip EnhancementDocument11 pagini"No-Touch" Technique For Lip EnhancementClaudia Antonia Ortiz Peralta0% (1)
- Multiple Microneedling Sessions For Minimally Invasive FacialDocument9 paginiMultiple Microneedling Sessions For Minimally Invasive FacialludyÎncă nu există evaluări
- Topographic Anatomy of The Superior Labial Artery For Dermal Filler Injection - Lee, 2014Document6 paginiTopographic Anatomy of The Superior Labial Artery For Dermal Filler Injection - Lee, 2014Rafael Autran Cavalcante AraújoÎncă nu există evaluări
- Clinical Anatomy and Regional PDFDocument24 paginiClinical Anatomy and Regional PDFChris LicínioÎncă nu există evaluări
- Effect of Kinesiology Taping On Breast Cancer Related Lymphedema A Randomized Singles Blind Controlled Pilot StudyDocument8 paginiEffect of Kinesiology Taping On Breast Cancer Related Lymphedema A Randomized Singles Blind Controlled Pilot StudyCesar C SÎncă nu există evaluări
- UntitledDocument147 paginiUntitledRianna MariaÎncă nu există evaluări
- The History of Botulinum Toxin From Poison To BeautyDocument3 paginiThe History of Botulinum Toxin From Poison To BeautyElaine MedeirosÎncă nu există evaluări
- Physical Means of Treating Unwanted Hair: R W & T S. ADocument10 paginiPhysical Means of Treating Unwanted Hair: R W & T S. Adipika awindaÎncă nu există evaluări
- Calcium HydroxylapatiteDocument4 paginiCalcium HydroxylapatiteBalance E-zineÎncă nu există evaluări
- Dermatology BookDocument13 paginiDermatology BookYezenashÎncă nu există evaluări
- Medische Peeling AlternatiefDocument33 paginiMedische Peeling AlternatiefERICSON LABORATOIRE100% (2)
- PRS 2015 01 SykesDocument15 paginiPRS 2015 01 Sykespsdsportsdoc100% (2)
- Lipolytic Laser: Price, Effectiveness and ContraindicationsDocument1 paginăLipolytic Laser: Price, Effectiveness and ContraindicationsDaniel Fajardo VilacháÎncă nu există evaluări
- Aesthetic Durable Forehead Contouring in Asians With Fat Grafting and Botulinum ToxinDocument7 paginiAesthetic Durable Forehead Contouring in Asians With Fat Grafting and Botulinum ToxinAnonymous LnWIBo1GÎncă nu există evaluări
- Literature Review of Cosmetic Procedures in Men Approaches and Techniques Are Gender SpecificDocument10 paginiLiterature Review of Cosmetic Procedures in Men Approaches and Techniques Are Gender SpecificImanuel Cristianto100% (1)
- Aesthetic Injection: Dr. Ersje Retnowati, M.BiomedDocument53 paginiAesthetic Injection: Dr. Ersje Retnowati, M.Biomedmohammad.irfanÎncă nu există evaluări
- Acido GlicolicoDocument4 paginiAcido GlicolicoRojas Evert AlonsoÎncă nu există evaluări
- Anatomia FeteiDocument32 paginiAnatomia FeteiPascalau AndreiÎncă nu există evaluări
- Facial Arterial Depth and Relationship With The Facial Musculature Layer - Lee, 2014Document8 paginiFacial Arterial Depth and Relationship With The Facial Musculature Layer - Lee, 2014Rafael Autran Cavalcante AraújoÎncă nu există evaluări
- FaceAXS+Slim+User ManualDocument51 paginiFaceAXS+Slim+User ManualAdrian LopezÎncă nu există evaluări
- Décolletage: Regional Approaches With Injectable FillersDocument6 paginiDécolletage: Regional Approaches With Injectable Fillersdanielagonzalezt5Încă nu există evaluări
- Tailored Injection Techniques in The Mid and Lower Face Using A Multilayering ApproachDocument9 paginiTailored Injection Techniques in The Mid and Lower Face Using A Multilayering Approachalh basharÎncă nu există evaluări
- CP 111Document246 paginiCP 111Yhr YhÎncă nu există evaluări
- A Modified Technique For Removing Earlobe KeloidsDocument3 paginiA Modified Technique For Removing Earlobe KeloidsdoctorbanÎncă nu există evaluări
- Facial MesotherapyDocument3 paginiFacial Mesotherapydanielagonzalezt5Încă nu există evaluări
- Your Hyperpigmentation E-BookDocument10 paginiYour Hyperpigmentation E-BookN SubhashÎncă nu există evaluări
- P ('t':'3', 'I':'173837501') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Document9 paginiP ('t':'3', 'I':'173837501') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Renobulan Sanusi0% (1)
- Influencia Del Betacaroteno en FumadoresDocument8 paginiInfluencia Del Betacaroteno en FumadoresHugh MantaÎncă nu există evaluări
- Ali 2018Document35 paginiAli 2018Hugh MantaÎncă nu există evaluări
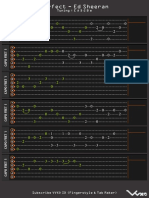
- Perfect TABDocument4 paginiPerfect TABMateus Gheorghiu100% (1)
- 2016 HandbookOfMaleicAnhydrideBased PDFDocument642 pagini2016 HandbookOfMaleicAnhydrideBased PDFAnonymous 0doDAL1100% (1)
- (BP Process Safety Series) BP Safety Group-Safe Furnace and Boiler Firing-Institution of Chemical Engineers (IChemE) (2005) PDFDocument86 pagini(BP Process Safety Series) BP Safety Group-Safe Furnace and Boiler Firing-Institution of Chemical Engineers (IChemE) (2005) PDFHugh MantaÎncă nu există evaluări
- Car Care Eng A4 2010-09 v3Document8 paginiCar Care Eng A4 2010-09 v3John J Cadavid100% (2)
- Canine Distemper 1Document12 paginiCanine Distemper 1Hugh MantaÎncă nu există evaluări
- Surfactants MOS - Jan 2009Document43 paginiSurfactants MOS - Jan 2009Antonio J PurielÎncă nu există evaluări
- Equilibar EVR VacuumDocument7 paginiEquilibar EVR VacuumHugh MantaÎncă nu există evaluări
- Fenton Consumo Electrico PDFDocument8 paginiFenton Consumo Electrico PDFHugh MantaÎncă nu există evaluări
- D2073 Total Primary Secondary and Tertiary Amine Values ofDocument3 paginiD2073 Total Primary Secondary and Tertiary Amine Values ofRAZA MEHDIÎncă nu există evaluări
- Manómetros Con Sifón y Válvula-Instrucciones de Instalación y MantenimientoDocument1 paginăManómetros Con Sifón y Válvula-Instrucciones de Instalación y MantenimientoHugh MantaÎncă nu există evaluări
- A Review On Lycopene-Extraction, Purification, Stability and ApplicationsDocument11 paginiA Review On Lycopene-Extraction, Purification, Stability and ApplicationsHugh MantaÎncă nu există evaluări
- GBH Enterprises, LTD.: Process DisclaimerDocument37 paginiGBH Enterprises, LTD.: Process DisclaimerAshwin ChandaranaÎncă nu există evaluări
- Next Generation Oleo & SurfactantDocument18 paginiNext Generation Oleo & SurfactantHugh MantaÎncă nu există evaluări
- Wang RotorDocument8 paginiWang RotorHugh MantaÎncă nu există evaluări
- Caninedistemper1 PDFDocument6 paginiCaninedistemper1 PDFHugh MantaÎncă nu există evaluări
- DURLON RR TANKCAR February 2015Document16 paginiDURLON RR TANKCAR February 2015Hugh Manta100% (1)
- Heating Failure Detection PDFDocument3 paginiHeating Failure Detection PDFHugh MantaÎncă nu există evaluări
- Melasma: A Comprehensive Update: Ontinuing Medical EducationDocument9 paginiMelasma: A Comprehensive Update: Ontinuing Medical EducationHugh MantaÎncă nu există evaluări
- A Ferrous Oxalate Mediated Photo-Fenton System: Toward An Increased Biodegradability of Índigo Dyed WastewatersDocument10 paginiA Ferrous Oxalate Mediated Photo-Fenton System: Toward An Increased Biodegradability of Índigo Dyed WastewatersHugh MantaÎncă nu există evaluări
- Vectra XL BrochureDocument4 paginiVectra XL BrochureMarcio SilvaÎncă nu există evaluări
- Methanol Safe Handling Manual Oct 2008 Spanish Eb42Document9 paginiMethanol Safe Handling Manual Oct 2008 Spanish Eb42Hugh MantaÎncă nu există evaluări
- Zahida Bouzina, Ilham Mokbel, Amina Negadi, Jacques Jose, Latifa NegadiDocument12 paginiZahida Bouzina, Ilham Mokbel, Amina Negadi, Jacques Jose, Latifa NegadiHugh MantaÎncă nu există evaluări
- Toxicological Profiles AmmoniaDocument248 paginiToxicological Profiles AmmoniaHugh MantaÎncă nu există evaluări
- Morofolina Conductividad PDFDocument1 paginăMorofolina Conductividad PDFHugh MantaÎncă nu există evaluări
- Student Projects For Distillation PDFDocument186 paginiStudent Projects For Distillation PDFHugh Manta100% (2)
- Tank Lining Brochure - PL - 20140625 PDFDocument7 paginiTank Lining Brochure - PL - 20140625 PDFfbraysÎncă nu există evaluări
- PreparingAerogels PDFDocument9 paginiPreparingAerogels PDFHugh MantaÎncă nu există evaluări
- When SIBO & IBS-Constipation Are Just Unrecognized Thiamine DeficiencyDocument3 paginiWhen SIBO & IBS-Constipation Are Just Unrecognized Thiamine Deficiencyps piasÎncă nu există evaluări
- What Is The Difference Between Newtonian and Non-Newtonian Fluid and Give Example For Each Case?Document11 paginiWhat Is The Difference Between Newtonian and Non-Newtonian Fluid and Give Example For Each Case?MOHAMED ABD ELGHANYÎncă nu există evaluări
- Pull Cord Switch JayashreeDocument1 paginăPull Cord Switch JayashreeNCÎncă nu există evaluări
- Book Chapter 11 SubmissionDocument18 paginiBook Chapter 11 Submissioncristine_2006_g5590Încă nu există evaluări
- Chapter 9Document28 paginiChapter 9Aniket BatraÎncă nu există evaluări
- Maskote WB Zinc Stop-OffDocument7 paginiMaskote WB Zinc Stop-OffbondsivamaniÎncă nu există evaluări
- Swiss Army Triplet 1Document2 paginiSwiss Army Triplet 1johnpwayÎncă nu există evaluări
- Dragons ScaleDocument13 paginiDragons ScaleGuilherme De FariasÎncă nu există evaluări
- Matutum View Academy: (The School of Faith)Document14 paginiMatutum View Academy: (The School of Faith)Neil Trezley Sunico BalajadiaÎncă nu există evaluări
- High Speed Power TransferDocument33 paginiHigh Speed Power TransferJAYKUMAR SINGHÎncă nu există evaluări
- Nursing Assessment in Family Nursing PracticeDocument22 paginiNursing Assessment in Family Nursing PracticeHydra Olivar - PantilganÎncă nu există evaluări
- Chapter 3 Extension - Game Theory-StDocument25 paginiChapter 3 Extension - Game Theory-StQuynh Chau TranÎncă nu există evaluări
- SRS For Travel AgencyDocument5 paginiSRS For Travel AgencyHardik SawalsaÎncă nu există evaluări
- Chudamani Women Expecting ChangeDocument55 paginiChudamani Women Expecting ChangeMr AnantÎncă nu există evaluări
- Teaching PowerPoint Slides - Chapter 5Document19 paginiTeaching PowerPoint Slides - Chapter 5Azril ShazwanÎncă nu există evaluări
- Lesson Plan 1Document3 paginiLesson Plan 1api-311983208Încă nu există evaluări
- The Other Twelve Part 1Document5 paginiThe Other Twelve Part 1vv380100% (2)
- Iso 22301 2019 en PDFDocument11 paginiIso 22301 2019 en PDFImam Saleh100% (3)
- Nails Care: Word Search: Name: - DateDocument1 paginăNails Care: Word Search: Name: - DateDeverly Hernandez Balba-AmplayoÎncă nu există evaluări
- Catalogue - Central Battery SystemDocument12 paginiCatalogue - Central Battery SystemarifzakirÎncă nu există evaluări
- Review Course 2 (Review On Professional Education Courses)Document8 paginiReview Course 2 (Review On Professional Education Courses)Regie MarcosÎncă nu există evaluări
- DeadlocksDocument41 paginiDeadlocksSanjal DesaiÎncă nu există evaluări
- Big Brother Naija and Its Impact On Nigeria University Students 2 PDFDocument30 paginiBig Brother Naija and Its Impact On Nigeria University Students 2 PDFIlufoye Tunde100% (1)
- Sips 1328Document64 paginiSips 1328Jean Claude De AldánÎncă nu există evaluări
- Baby DedicationDocument3 paginiBaby DedicationLouriel Nopal100% (3)
- Fellows (Antiques)Document90 paginiFellows (Antiques)messapos100% (1)
- Lecture BouffonDocument1 paginăLecture BouffonCarlos Enrique GuerraÎncă nu există evaluări
- Using Your Digital Assets On Q-GlobalDocument3 paginiUsing Your Digital Assets On Q-GlobalRemik BuczekÎncă nu există evaluări
- UpdateJul2007 3julDocument10 paginiUpdateJul2007 3julAnshul SinghÎncă nu există evaluări
- QF Jacket (Drafting & Cutting) - GAR620Document15 paginiQF Jacket (Drafting & Cutting) - GAR620abdulraheem18822Încă nu există evaluări
- The Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyDe la EverandThe Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyÎncă nu există evaluări
- Forever Strong: A New, Science-Based Strategy for Aging WellDe la EverandForever Strong: A New, Science-Based Strategy for Aging WellÎncă nu există evaluări
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookDe la EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookEvaluare: 3.5 din 5 stele3.5/5 (2)
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)De la EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Evaluare: 4 din 5 stele4/5 (378)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisDe la EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisEvaluare: 3 din 5 stele3/5 (2)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyDe la EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyEvaluare: 4.5 din 5 stele4.5/5 (2)
- Eat & Run: My Unlikely Journey to Ultramarathon GreatnessDe la EverandEat & Run: My Unlikely Journey to Ultramarathon GreatnessÎncă nu există evaluări
- Summary of Mary Claire Haver's The Galveston DietDe la EverandSummary of Mary Claire Haver's The Galveston DietEvaluare: 5 din 5 stele5/5 (1)
- The Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingDe la EverandThe Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingEvaluare: 4 din 5 stele4/5 (3)
- Sugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthDe la EverandSugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthEvaluare: 4 din 5 stele4/5 (6)
- Hungry for Change: Ditch the Diets, Conquer the Cravings, and Eat Your Way to Lifelong HealthDe la EverandHungry for Change: Ditch the Diets, Conquer the Cravings, and Eat Your Way to Lifelong HealthEvaluare: 4 din 5 stele4/5 (7)
- How Not to Die by Michael Greger MD, Gene Stone - Book Summary: Discover the Foods Scientifically Proven to Prevent and Reverse DiseaseDe la EverandHow Not to Die by Michael Greger MD, Gene Stone - Book Summary: Discover the Foods Scientifically Proven to Prevent and Reverse DiseaseEvaluare: 4.5 din 5 stele4.5/5 (83)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeDe la EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeÎncă nu există evaluări
- Keto Friendly Recipes: Easy Keto For Busy PeopleDe la EverandKeto Friendly Recipes: Easy Keto For Busy PeopleEvaluare: 3.5 din 5 stele3.5/5 (2)
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonDe la EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonEvaluare: 3.5 din 5 stele3.5/5 (33)
- Eat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouDe la EverandEat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouÎncă nu există evaluări
- Find Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeDe la EverandFind Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeEvaluare: 4 din 5 stele4/5 (3)
- Secrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainDe la EverandSecrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainEvaluare: 3.5 din 5 stele3.5/5 (38)
- How to Be Well: The 6 Keys to a Happy and Healthy LifeDe la EverandHow to Be Well: The 6 Keys to a Happy and Healthy LifeEvaluare: 5 din 5 stele5/5 (1)
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthDe la EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthÎncă nu există evaluări
- Grit & Grace: Train the Mind, Train the Body, Own Your LifeDe la EverandGrit & Grace: Train the Mind, Train the Body, Own Your LifeEvaluare: 4 din 5 stele4/5 (3)
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsDe la EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsEvaluare: 4 din 5 stele4/5 (49)
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomDe la EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomEvaluare: 4 din 5 stele4/5 (1)
- The Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodDe la EverandThe Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodÎncă nu există evaluări
- The Volumetrics Eating Plan: Techniques and Recipes for Feeling Full on Fewer CaloriesDe la EverandThe Volumetrics Eating Plan: Techniques and Recipes for Feeling Full on Fewer CaloriesÎncă nu există evaluări
- Intermittent Fasting Basics for Women: The Complete Guide to Safe and Effective Weight Loss with Intermittent FastingDe la EverandIntermittent Fasting Basics for Women: The Complete Guide to Safe and Effective Weight Loss with Intermittent FastingEvaluare: 5 din 5 stele5/5 (12)
- Happy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainDe la EverandHappy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainEvaluare: 3.5 din 5 stele3.5/5 (6)
- Glucose Revolution: The Life-Changing Power of Balancing Your Blood SugarDe la EverandGlucose Revolution: The Life-Changing Power of Balancing Your Blood SugarEvaluare: 5 din 5 stele5/5 (351)