S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- "Don't Say Gay" BillDocument4 pagini"Don't Say Gay" BillAdam PoulisseÎncă nu există evaluări
- Pharmacology Case Study 1 Acne VulgarisDocument6 paginiPharmacology Case Study 1 Acne Vulgarisapi-456313554Încă nu există evaluări
- High Blood Pressure ScreeningDocument10 paginiHigh Blood Pressure Screeningapi-456313554Încă nu există evaluări
- Matulichalyssan500 TheorycritiqueDocument5 paginiMatulichalyssan500 Theorycritiqueapi-456313554Încă nu există evaluări
- Running Head: High Blood Pressure Screening 1Document13 paginiRunning Head: High Blood Pressure Screening 1api-456313554Încă nu există evaluări
- Soap 3 Adult Alyssa MatulichDocument6 paginiSoap 3 Adult Alyssa Matulichapi-456313554Încă nu există evaluări
- Soap 2Document5 paginiSoap 2api-456313554Încă nu există evaluări
- Soap 3Document5 paginiSoap 3api-456313554Încă nu există evaluări
- Pre-Reflection Womens Health Paper Alyssa MatulichDocument5 paginiPre-Reflection Womens Health Paper Alyssa Matulichapi-456313554Încă nu există evaluări
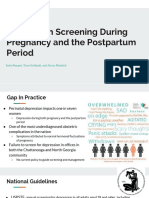
- Running Head: Depression Screening 1Document26 paginiRunning Head: Depression Screening 1api-456313554Încă nu există evaluări
- BurgettDocument10 paginiBurgettapi-456313554Încă nu există evaluări
- Treatment Protocol Migraine ProphylaxisDocument2 paginiTreatment Protocol Migraine Prophylaxisapi-456313554Încă nu există evaluări
- UTC SON Health Clinic: Student Name: Alyssa Matulich Date: 3/12/19Document5 paginiUTC SON Health Clinic: Student Name: Alyssa Matulich Date: 3/12/19api-456313554Încă nu există evaluări
- Soap Note 5 Acute - Alyssa MatulichDocument7 paginiSoap Note 5 Acute - Alyssa Matulichapi-456313554Încă nu există evaluări
- Cheal PaperDocument5 paginiCheal Paperapi-456313554Încă nu există evaluări
- Soap Note 2 Alyssa MatulichDocument8 paginiSoap Note 2 Alyssa Matulichapi-456313554Încă nu există evaluări
- Treatment Protocol Acute GoutDocument2 paginiTreatment Protocol Acute Goutapi-456313554Încă nu există evaluări
- Running Head: Pediatric Case Study: Scabies 1Document17 paginiRunning Head: Pediatric Case Study: Scabies 1api-456313554Încă nu există evaluări
- Whitney Social Studies SbaDocument23 paginiWhitney Social Studies SbaWhitney Ellington0% (1)
- Antenatal CareDocument11 paginiAntenatal CareKavitha pÎncă nu există evaluări
- Practical Training 2nd Memorial GargiDocument12 paginiPractical Training 2nd Memorial GargiIshan goyal100% (1)
- Chapter 7Document134 paginiChapter 7raguchandra7527Încă nu există evaluări
- Be It Enacted by The Senate and House of Representatives of The Philippines in Congress AssembledDocument14 paginiBe It Enacted by The Senate and House of Representatives of The Philippines in Congress AssembledFranz MaclangÎncă nu există evaluări
- Membership of School Council: NotificationDocument4 paginiMembership of School Council: NotificationAasif NawazÎncă nu există evaluări
- Family Law The Essentials 3rd Edition Statsky Test BankDocument4 paginiFamily Law The Essentials 3rd Edition Statsky Test Bankcoilwheyb7wsk100% (25)
- Bcal-3731 212621 7 Child Information RecordDocument1 paginăBcal-3731 212621 7 Child Information Recordapi-261936496Încă nu există evaluări
- ARNEC Connections 2011-Draft - BW - Web PDFDocument48 paginiARNEC Connections 2011-Draft - BW - Web PDFSithu WaiÎncă nu există evaluări
- Conflicts of Law Report On Marriage and AdoptionDocument50 paginiConflicts of Law Report On Marriage and AdoptionGail Fabroa NavarraÎncă nu există evaluări
- Adoption by Same-Sex Couples: Ketevan Kukhianidze, PHD StudentDocument7 paginiAdoption by Same-Sex Couples: Ketevan Kukhianidze, PHD StudentJohnny JohnnieeÎncă nu există evaluări
- Competition, Cooperation and Conflict in Economy and BiologyDocument7 paginiCompetition, Cooperation and Conflict in Economy and BiologyCarolina Riveros ArdilaÎncă nu există evaluări
- FAQs Solo Parent and Parental LeaveDocument3 paginiFAQs Solo Parent and Parental Leavemolv22Încă nu există evaluări
- Relationships by Sankhuleni PhiriDocument3 paginiRelationships by Sankhuleni PhiriWillsStudioÎncă nu există evaluări
- Gay Parenthood and The Decline of Paternity As We Knew ItDocument30 paginiGay Parenthood and The Decline of Paternity As We Knew ItAPÎncă nu există evaluări
- Adoption PresentationDocument49 paginiAdoption PresentationAnupam ThakurÎncă nu există evaluări
- 100 Band 7, 8 + 9 IELTS Writing Task 2 Essay Samples - IELTS AdvantageDocument1 pagină100 Band 7, 8 + 9 IELTS Writing Task 2 Essay Samples - IELTS Advantageohohfh432Încă nu există evaluări
- Pil 50 IDocument6 paginiPil 50 IKiran kumarÎncă nu există evaluări
- Lesson 1 - KinshipDocument2 paginiLesson 1 - KinshipGlester SevillaÎncă nu există evaluări
- CIY Move 2008 Info PacketDocument5 paginiCIY Move 2008 Info Packetlarue23Încă nu există evaluări
- Little Essays of Love and Virtue by Ellis, Havelock, 1859-1939Document69 paginiLittle Essays of Love and Virtue by Ellis, Havelock, 1859-1939Gutenberg.orgÎncă nu există evaluări
- Network Responsibility FormsDocument2 paginiNetwork Responsibility Formscj1900Încă nu există evaluări
- Refusal To Be TransferredDocument2 paginiRefusal To Be TransferredIsabella RodriguezÎncă nu există evaluări
- Reflection Paper #1 FAMIPOPDocument1 paginăReflection Paper #1 FAMIPOPMico LapuzÎncă nu există evaluări
- Vancil vs. Belmes Case DigestDocument5 paginiVancil vs. Belmes Case DigestrfylananÎncă nu există evaluări
- Sina-On, Glennie - Critical Essay - Final Paper For HE 290ADocument9 paginiSina-On, Glennie - Critical Essay - Final Paper For HE 290AGlennieMarieSina-onÎncă nu există evaluări
- Mah 3Document2 paginiMah 3Ceejay Decena PasicolanÎncă nu există evaluări
- Michigan Federal Child Welfare Modified Settlement AgreementDocument58 paginiMichigan Federal Child Welfare Modified Settlement AgreementBeverly TranÎncă nu există evaluări
- Ethical Issues About Genetic TestingDocument4 paginiEthical Issues About Genetic Testingjeidre pamorcaÎncă nu există evaluări