S-ar putea să vă placă și
- Case Sutdy - LymphomaDocument54 paginiCase Sutdy - LymphomaGrasyang FernandezÎncă nu există evaluări
- Pulmonary TuberculosisDocument28 paginiPulmonary TuberculosisKoRnflakes86% (14)
- Anatomy, Physiology and Pathology of The RespiratoryDocument68 paginiAnatomy, Physiology and Pathology of The Respiratorytheresia_s_k100% (1)
- UTIDocument43 paginiUTIGrasyang FernandezÎncă nu există evaluări
- DEDICATION and AcknowledmentDocument2 paginiDEDICATION and AcknowledmentGrasyang FernandezÎncă nu există evaluări
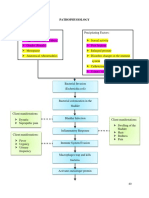
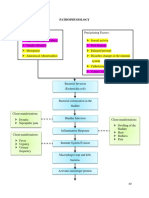
- PathophysiologyDocument3 paginiPathophysiologyGrasyang FernandezÎncă nu există evaluări
- Path o PhysiologyDocument3 paginiPath o PhysiologyGrasyang FernandezÎncă nu există evaluări
- REPORT LeadershipDocument20 paginiREPORT LeadershipGrasyang FernandezÎncă nu există evaluări
- UTIDocument59 paginiUTIGrasyang FernandezÎncă nu există evaluări
- UTIDocument59 paginiUTIGrasyang FernandezÎncă nu există evaluări
- Patient Health HistoryDocument2 paginiPatient Health HistoryGrasyang FernandezÎncă nu există evaluări
- Patient Health HistoryDocument2 paginiPatient Health HistoryGrasyang FernandezÎncă nu există evaluări
- Regional Divisions of China HistoryDocument15 paginiRegional Divisions of China HistoryGrasyang FernandezÎncă nu există evaluări
- Chemistry For EngineersDocument5 paginiChemistry For EngineersGrasyang FernandezÎncă nu există evaluări
- CatheterizationDocument5 paginiCatheterizationGrasyang FernandezÎncă nu există evaluări
- CatheterizationDocument5 paginiCatheterizationGrasyang FernandezÎncă nu există evaluări
- CatheterizationDocument5 paginiCatheterizationGrasyang FernandezÎncă nu există evaluări
- NilliekkkkkkkDocument58 paginiNilliekkkkkkkGrasyang FernandezÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Clinical Sheets 2Document38 paginiClinical Sheets 2FathiBestÎncă nu există evaluări
- 3 PDFDocument2 pagini3 PDFKrupali JainÎncă nu există evaluări
- NICU Survival GuideDocument14 paginiNICU Survival Guidesedaka26Încă nu există evaluări
- PLM-CM Marsf Booksale'09Document2 paginiPLM-CM Marsf Booksale'09m0rinskiÎncă nu există evaluări
- BreastfeedingDocument13 paginiBreastfeedingSintya AulinaÎncă nu există evaluări
- Trauma Team Roles1Document12 paginiTrauma Team Roles1affanÎncă nu există evaluări
- Xantoma Semj-16-07-29569Document5 paginiXantoma Semj-16-07-29569Agus SyaifudinÎncă nu există evaluări
- Shredder Capacity - Bio Medical WasteDocument3 paginiShredder Capacity - Bio Medical WasteYasser FathiÎncă nu există evaluări
- 11 Self EsteemDocument16 pagini11 Self EsteemPrettyAnnie51100% (1)
- Resume of MzeiseDocument6 paginiResume of Mzeiseapi-27610566Încă nu există evaluări
- Evidence Based Practice PaperDocument9 paginiEvidence Based Practice Paperapi-403588433Încă nu există evaluări
- Policy On Pediatric Dental Pain ManagementDocument3 paginiPolicy On Pediatric Dental Pain ManagementمعتزباللهÎncă nu există evaluări
- Peptic Ulcer Disease Guidline Univ of Michigan Health System PDFDocument7 paginiPeptic Ulcer Disease Guidline Univ of Michigan Health System PDFsyafiraÎncă nu există evaluări
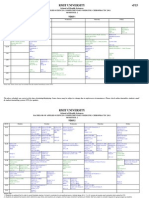
- Sem2 TimetableDocument5 paginiSem2 Timetablemasso23684Încă nu există evaluări
- Dosage CalculationsDocument39 paginiDosage Calculationssalak9462900% (1)
- Surgery 2Document27 paginiSurgery 2junaid4shaikhÎncă nu există evaluări
- 2010 MGMA Physician Compensation Survey SummaryDocument7 pagini2010 MGMA Physician Compensation Survey Summaryjoespromos100% (1)
- 31412Document369 pagini31412aptureinc100% (5)
- Acute Upper Airway Obstruction in Children: Paediatric Anaesthesia Tutorial 368Document9 paginiAcute Upper Airway Obstruction in Children: Paediatric Anaesthesia Tutorial 368Fireka JuniantikaÎncă nu există evaluări
- Pedia Notes Compiled PDFDocument133 paginiPedia Notes Compiled PDFAljeirou AlcachupasÎncă nu există evaluări
- National Urban Health MissionDocument7 paginiNational Urban Health MissionSudhakar AnandÎncă nu există evaluări
- 2010 Abstract SupplementDocument360 pagini2010 Abstract SupplementcatatanÎncă nu există evaluări
- COVID Toes, Rashes: How The Coronavirus Can Affect Your SkinDocument6 paginiCOVID Toes, Rashes: How The Coronavirus Can Affect Your SkinlittlemisseeeÎncă nu există evaluări
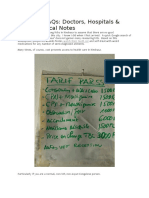
- Kinshasa FAQs - HopitauxDocument15 paginiKinshasa FAQs - HopitauxJoelLadjoÎncă nu există evaluări
- 16 Bier BlockDocument28 pagini16 Bier BlockJessica CÎncă nu există evaluări
- Neuroanatomy Laboratory Guide 2011Document8 paginiNeuroanatomy Laboratory Guide 2011Steve BlubaughÎncă nu există evaluări
- Prev Med and Public Health Review ExamDocument6 paginiPrev Med and Public Health Review ExamRosel Ann BontiaÎncă nu există evaluări
- Prophylaxis and Treatment For AspirationDocument19 paginiProphylaxis and Treatment For Aspirationbalab2311Încă nu există evaluări
- Recent Development of Travel Medicine: Current Issues Prof. Dr. Soesanto Tjokrosonto 2006Document28 paginiRecent Development of Travel Medicine: Current Issues Prof. Dr. Soesanto Tjokrosonto 2006Red DemonÎncă nu există evaluări
- Mindray UMEC 12 Specifications FDADocument11 paginiMindray UMEC 12 Specifications FDAAlejandra Baas GuzmánÎncă nu există evaluări