S-ar putea să vă placă și
- The Link between Nutrition, Glutathione and Covid-19: What They May Not Have Told YouDe la EverandThe Link between Nutrition, Glutathione and Covid-19: What They May Not Have Told YouÎncă nu există evaluări
- Prospective, Randomized Clinical Trial ofDocument10 paginiProspective, Randomized Clinical Trial ofFarhan RezaÎncă nu există evaluări
- Schechter 2015Document8 paginiSchechter 2015joseph rivaldoÎncă nu există evaluări
- Association Between Early Life Antibiotic Exposure and Development of Early Childhood Atopic DermatitisDocument7 paginiAssociation Between Early Life Antibiotic Exposure and Development of Early Childhood Atopic DermatitismunadocumÎncă nu există evaluări
- Key Components For Antibiotic Dose Optimization of Sepsis in Neonates and InfantsDocument9 paginiKey Components For Antibiotic Dose Optimization of Sepsis in Neonates and InfantsDendi HidayatullahÎncă nu există evaluări
- The Use of Antimicrobial Peptides in Ophthalmology: An Experimental Study in Corneal Preservation and The Management of Bacterial KeratitisDocument30 paginiThe Use of Antimicrobial Peptides in Ophthalmology: An Experimental Study in Corneal Preservation and The Management of Bacterial KeratitisAgam ThebadboysÎncă nu există evaluări
- Analysis: The Antibiotic Course Has Had Its DayDocument5 paginiAnalysis: The Antibiotic Course Has Had Its Daysimx88Încă nu există evaluări
- Intravitreal Injections Primary Prevention: A Case-Control StudyDocument6 paginiIntravitreal Injections Primary Prevention: A Case-Control StudyZipippo ZÎncă nu există evaluări
- Antibacterial and Anti-Inflammatory Activities of 4-Hydroxycordoin: Potential Therapeutic BenefitsDocument6 paginiAntibacterial and Anti-Inflammatory Activities of 4-Hydroxycordoin: Potential Therapeutic BenefitsVinícius PiantaÎncă nu există evaluări
- J Ajo 2020 03 018Document24 paginiJ Ajo 2020 03 018koas forensikÎncă nu există evaluări
- FFHGDDGHCSFGDocument2 paginiFFHGDDGHCSFGनटराज नचिकेताÎncă nu există evaluări
- Povidone Iodine: Useful For More Than Preoperative AntisepsisDocument4 paginiPovidone Iodine: Useful For More Than Preoperative AntisepsisNur AjiÎncă nu există evaluări
- BQL RX ConsDocument3 paginiBQL RX ConsAwe Angga WirahmadiÎncă nu există evaluări
- Proceedings of The 14th European Immunogenicity Platform Open Symposium On Immunogenicity of BiopharmaceuticalsDocument8 paginiProceedings of The 14th European Immunogenicity Platform Open Symposium On Immunogenicity of Biopharmaceuticalsgskcl429Încă nu există evaluări
- Accepted Manuscript: 10.1016/j.ajo.2016.10.004Document22 paginiAccepted Manuscript: 10.1016/j.ajo.2016.10.004benefits35Încă nu există evaluări
- Kanagalingam2015 PDFDocument10 paginiKanagalingam2015 PDFwatidinaÎncă nu există evaluări
- A Possible Alternative and Safe Adjunctive Role Forlocally Appliedmangiferinin Periodontal Therapy A Clinical and Microbiological StudyDocument15 paginiA Possible Alternative and Safe Adjunctive Role Forlocally Appliedmangiferinin Periodontal Therapy A Clinical and Microbiological StudyIJAR JOURNALÎncă nu există evaluări
- Safety Aspects of Probiotic ProductsDocument4 paginiSafety Aspects of Probiotic ProductsSrinivas PingaliÎncă nu există evaluări
- Editorial: Decisions and Antibiotics Use: More Questions and Some AnswersDocument3 paginiEditorial: Decisions and Antibiotics Use: More Questions and Some AnswersTommy Leon SilvaÎncă nu există evaluări
- Wound 2016 0701Document9 paginiWound 2016 0701Ine Marthia DanieÎncă nu există evaluări
- The Latest Updates and Management of Endophthalmitis: DitorialDocument4 paginiThe Latest Updates and Management of Endophthalmitis: Ditorialtaufik perdanaÎncă nu există evaluări
- Immunological Reviews - 2019 - Kurtovic - Complement in Malaria Immunity and VaccinesDocument19 paginiImmunological Reviews - 2019 - Kurtovic - Complement in Malaria Immunity and VaccinesFaiz SheeÎncă nu există evaluări
- Pharmatutor: Edible Vaccine - A Great Boon in Medicinal ScienceDocument4 paginiPharmatutor: Edible Vaccine - A Great Boon in Medicinal ScienceShailendra YadavÎncă nu există evaluări
- Microbial Keratitis and The Selection of Topical AntimicrobialsDocument2 paginiMicrobial Keratitis and The Selection of Topical AntimicrobialsAriyoko PatodingÎncă nu există evaluări
- BP AntibiotictherapyDocument5 paginiBP AntibiotictherapyViiial CoÎncă nu există evaluări
- Antimicrobial Resistance ThesisDocument5 paginiAntimicrobial Resistance Thesissheenacrouchmurfreesboro100% (1)
- Theresa S. Samaniego Philippine Daily InquirerDocument4 paginiTheresa S. Samaniego Philippine Daily InquirerGolda-Fiel Tolentino LanguisanÎncă nu există evaluări
- Articulo ImpetigoDocument9 paginiArticulo ImpetigoAnahi GuerreroÎncă nu există evaluări
- Topical and Systemic Antibiotics in The Management of Periodontal DiseasesDocument12 paginiTopical and Systemic Antibiotics in The Management of Periodontal DiseasesxdxdxdxdÎncă nu există evaluări
- MK in PediDocument7 paginiMK in PedifikerteadelleÎncă nu există evaluări
- 1 jISHADocument5 pagini1 jISHAFirman MufidÎncă nu există evaluări
- BP AntibiotictherapyDocument4 paginiBP AntibiotictherapyDebasmita Datta GuptaÎncă nu există evaluări
- International Wound Journal - 2018 - Percival - Role of Anaerobes in Polymicrobial Communities and Biofilms ComplicatingDocument7 paginiInternational Wound Journal - 2018 - Percival - Role of Anaerobes in Polymicrobial Communities and Biofilms ComplicatingIdamelis Rodríguez GarcíaÎncă nu există evaluări
- Check Unit 555 November Immunology V3 PDFDocument25 paginiCheck Unit 555 November Immunology V3 PDFdragon66Încă nu există evaluări
- Roth 1999Document20 paginiRoth 1999Sílvia BastosÎncă nu există evaluări
- New Treatments For Bacterial KeratitisDocument8 paginiNew Treatments For Bacterial KeratitisMuhamad Chairul SyahÎncă nu există evaluări
- Antibiotic Resistance: A Common Challenge in DentistryDocument6 paginiAntibiotic Resistance: A Common Challenge in DentistryIJAR JOURNALÎncă nu există evaluări
- Impetigo and Scabies e Disease Burden and Modern Treatment StrategiesDocument7 paginiImpetigo and Scabies e Disease Burden and Modern Treatment StrategiesHandy NugrahaÎncă nu există evaluări
- A National Online Survey of Filipinos' Knowledge, Attitude, and Awareness of Antibiotic Use and ResistanceDocument15 paginiA National Online Survey of Filipinos' Knowledge, Attitude, and Awareness of Antibiotic Use and Resistancerizal angeloÎncă nu există evaluări
- The Need For Another Typhoid Fever Vaccine: EditorialcommentaryDocument3 paginiThe Need For Another Typhoid Fever Vaccine: Editorialcommentaryshelly_shellyÎncă nu există evaluări
- Jurnal EED 3Document10 paginiJurnal EED 3Garsa GarnolÎncă nu există evaluări
- Phage TheoryDocument10 paginiPhage TheoryRudransh NaredaÎncă nu există evaluări
- Research Paper Antibiotic ResistanceDocument5 paginiResearch Paper Antibiotic Resistancegvyns594100% (1)
- Alimentação EscolarDocument8 paginiAlimentação EscolarFabi RamosÎncă nu există evaluări
- The New Zealand Medical JournalDocument7 paginiThe New Zealand Medical JournalNafhyraJunetÎncă nu există evaluări
- Jurnal Mata 1Document9 paginiJurnal Mata 1marhayudi15Încă nu există evaluări
- Pharmaceutics 14 01678Document14 paginiPharmaceutics 14 01678Ana ApolinárioÎncă nu există evaluări
- Vaccine Adjuvants: Current State and Future Trends: Special FeatureDocument9 paginiVaccine Adjuvants: Current State and Future Trends: Special Feature99manu99Încă nu există evaluări
- Cuppa Wao Journal ProofsDocument22 paginiCuppa Wao Journal ProofsFajar SetiawanÎncă nu există evaluări
- Artritis Juvenil Articulo CynthiaDocument15 paginiArtritis Juvenil Articulo CynthiaCynthia Adrianna Graciano EspinozaÎncă nu există evaluări
- ResearchDocument31 paginiResearchAlexa BarnÎncă nu există evaluări
- Research Paper On Antibiotic Resistance PDFDocument6 paginiResearch Paper On Antibiotic Resistance PDFgw1gnz6b100% (1)
- Where We AreDocument8 paginiWhere We AreHusna NadiaÎncă nu există evaluări
- Appropriate Use of Antibiotics in The NICUDocument6 paginiAppropriate Use of Antibiotics in The NICUmoniaÎncă nu există evaluări
- Potential Properties of Lactobacillus Plantarum F-10 As A Bio-Control Strategy For Wound InfectionsDocument14 paginiPotential Properties of Lactobacillus Plantarum F-10 As A Bio-Control Strategy For Wound InfectionsIgor BaltaÎncă nu există evaluări
- An Asian Perspective On Povidone Iodine in Wound Healing: Review PaperDocument2 paginiAn Asian Perspective On Povidone Iodine in Wound Healing: Review PaperDanisa AzzahraÎncă nu există evaluări
- Jurnal MataDocument28 paginiJurnal MatamarinatamiÎncă nu există evaluări
- Journ 3Document7 paginiJourn 3Yanasta Yudo PratamaÎncă nu există evaluări
- Use of Antibiotic Therapy For Pediatric Dental Patients: Latest RevisionDocument4 paginiUse of Antibiotic Therapy For Pediatric Dental Patients: Latest Revisionnona aryanÎncă nu există evaluări
- PLSC 207 PresentationDocument10 paginiPLSC 207 Presentationapi-534590324Încă nu există evaluări
- Gall 2013Document2 paginiGall 2013wawan 88Încă nu există evaluări
- Ghiam, Xu, Berry - 2019 - Aqueous Humor Markers in Retinoblastoma, A ReviewDocument15 paginiGhiam, Xu, Berry - 2019 - Aqueous Humor Markers in Retinoblastoma, A Reviewwawan 88Încă nu există evaluări
- Gekeler 2012Document1 paginăGekeler 2012wawan 88Încă nu există evaluări
- Entro OpDocument6 paginiEntro Opwawan 88Încă nu există evaluări
- Biostatistics Notes - Ico 2018Document17 paginiBiostatistics Notes - Ico 2018wawan 88Încă nu există evaluări
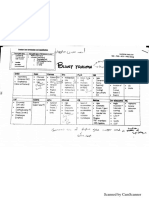
- TraumaDocument15 paginiTraumawawan 88Încă nu există evaluări
- Errors Mind MapDocument6 paginiErrors Mind Mapwawan 88Încă nu există evaluări
- 2007 LaiDocument36 pagini2007 Laiwawan 88Încă nu există evaluări
- Isolated Optic Perineuritis As The Presenting Sign of SarcoidosisDocument3 paginiIsolated Optic Perineuritis As The Presenting Sign of Sarcoidosiswawan 88Încă nu există evaluări
- Jurnal Katarak KongenitalDocument3 paginiJurnal Katarak KongenitalevajulitaÎncă nu există evaluări
- Surgical Management of Dilocated Lens: Mohammad Ghoreishi, MDDocument15 paginiSurgical Management of Dilocated Lens: Mohammad Ghoreishi, MDwawan 88Încă nu există evaluări
- SitasiDocument1 paginăSitasiwawan 88Încă nu există evaluări
- 50 Studies Questioning Vaccine SafetyDocument5 pagini50 Studies Questioning Vaccine SafetyshifanahmedÎncă nu există evaluări
- I Jos 201129Document9 paginiI Jos 201129jklhjÎncă nu există evaluări
- Symptoms of Bronchopneumonia in Adults and Children: PneumoniaDocument10 paginiSymptoms of Bronchopneumonia in Adults and Children: PneumoniajessyÎncă nu există evaluări
- Clinicopathologic Conference: Governor Celestino Gallares Memorial Hospital Department of Obstetrics and GynecologyDocument57 paginiClinicopathologic Conference: Governor Celestino Gallares Memorial Hospital Department of Obstetrics and GynecologyramwshÎncă nu există evaluări
- Os 1Document3 paginiOs 1rizwanÎncă nu există evaluări
- Dry Eye Disease After Refractive SurgeryDocument6 paginiDry Eye Disease After Refractive SurgeryCastiglianoÎncă nu există evaluări
- AIA HandbookDocument3 paginiAIA HandbookahmaddanialÎncă nu există evaluări
- Epidemiology, Risk Factors, Pathogenesis, and Natural History of Thoracic Aortic AneurysmDocument5 paginiEpidemiology, Risk Factors, Pathogenesis, and Natural History of Thoracic Aortic AneurysmNathaliazuosÎncă nu există evaluări
- Breastfeeding and Down SyndromeDocument239 paginiBreastfeeding and Down SyndromeSim M ChangÎncă nu există evaluări
- Paper 1 Bio Skills Practise 2023Document18 paginiPaper 1 Bio Skills Practise 2023nairamathrawala3000Încă nu există evaluări
- SAS 14 MCNDocument2 paginiSAS 14 MCNKristinelou Marie N. Reyna0% (1)
- Artificial or Supplimentary FoodDocument4 paginiArtificial or Supplimentary FoodArchana Sahu100% (1)
- Arlevert (Cinnarizinedimenhydrinate)Document2 paginiArlevert (Cinnarizinedimenhydrinate)zloncar3Încă nu există evaluări
- Opioid Adjuvant in NeuraxialDocument10 paginiOpioid Adjuvant in NeuraxialiswanlatifÎncă nu există evaluări
- Resusitasi NeonatusDocument7 paginiResusitasi NeonatusIqbal Miftahul HudaÎncă nu există evaluări
- Medicago Sativa LloydDocument4 paginiMedicago Sativa LloydDr Rushen SinghÎncă nu există evaluări
- Bird Mark 7A Respirator BrochureDocument2 paginiBird Mark 7A Respirator BrochureLos Infantes Ska Jazz100% (4)
- HSC4555 0001 Fall17 SyllabusDocument6 paginiHSC4555 0001 Fall17 SyllabusDilly RijoÎncă nu există evaluări
- Checklist - Assisting - Circulating DeliveryDocument2 paginiChecklist - Assisting - Circulating DeliveryLue Vigiem M. GuiasÎncă nu există evaluări
- Drug Study - LactuloseDocument1 paginăDrug Study - LactuloseCarla Tongson MaravillaÎncă nu există evaluări
- Purposive Communication - Writer: John Melvin Ibarra Type of Essay: Persuasive Instructor: Ms. Fhe de CastroDocument2 paginiPurposive Communication - Writer: John Melvin Ibarra Type of Essay: Persuasive Instructor: Ms. Fhe de CastroVincent Maralit Material100% (1)
- What Is-Thrombocythemia and ThrombocytosisDocument4 paginiWhat Is-Thrombocythemia and ThrombocytosisFred C. MirandaÎncă nu există evaluări
- Makalah Leigh Disease by Boys KDocument6 paginiMakalah Leigh Disease by Boys KAzizul HakimÎncă nu există evaluări
- Philippine College of Science and Technology College of NursingDocument21 paginiPhilippine College of Science and Technology College of NursingAijem RyanÎncă nu există evaluări
- Acute Complications of Diabetes Mellitus: Hypoglycemia and Hypoglycemic ComaDocument30 paginiAcute Complications of Diabetes Mellitus: Hypoglycemia and Hypoglycemic ComaCristinaGheorgheÎncă nu există evaluări
- Congenital Anomalies and Variations of The Bile and Pancreatic Ducts - Magnetic Resonance Cholangiopancreatography Findings, Epidemiology and Clinical SignificanceDocument19 paginiCongenital Anomalies and Variations of The Bile and Pancreatic Ducts - Magnetic Resonance Cholangiopancreatography Findings, Epidemiology and Clinical SignificanceRoberto HernandezÎncă nu există evaluări
- Teknik Operasi Splenektomi 2Document31 paginiTeknik Operasi Splenektomi 2sphericalfaÎncă nu există evaluări
- Hema - Guide Notes PDFDocument21 paginiHema - Guide Notes PDFVanessa Ladra100% (1)
- 32 Oet Reading Summary 2.0-697-717Document21 pagini32 Oet Reading Summary 2.0-697-717Santhus100% (7)
- Deficiencies Bariatric SurgeryDocument10 paginiDeficiencies Bariatric SurgeryYazen JoudehÎncă nu există evaluări