S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Rubrics For Skit or Role PlayDocument1 paginăRubrics For Skit or Role PlayGheyDelaCueva50% (2)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Escrow Agreement TemplateDocument5 paginiEscrow Agreement TemplatesamsarmaÎncă nu există evaluări
- Top 25 Test-Taking Tips, Suggestions & Strategies: WrongDocument5 paginiTop 25 Test-Taking Tips, Suggestions & Strategies: WronglheanzÎncă nu există evaluări
- MPCE 15 InternshipDocument56 paginiMPCE 15 InternshipRaghavÎncă nu există evaluări
- 2009-2014 Division of Student Affairs Strategic Plan: MissionDocument15 pagini2009-2014 Division of Student Affairs Strategic Plan: MissionDominicSavioÎncă nu există evaluări
- Tirupati Information PamphletDocument1 paginăTirupati Information PamphletsamsarmaÎncă nu există evaluări
- Presentation On AKGCo-1 FinalDocument40 paginiPresentation On AKGCo-1 FinalsamsarmaÎncă nu există evaluări
- Change of Land Use Policy Gazette Notification Andhra Pradesh CRDADocument4 paginiChange of Land Use Policy Gazette Notification Andhra Pradesh CRDAsamsarmaÎncă nu există evaluări
- Kadapa District Industries Profile MSMEDocument20 paginiKadapa District Industries Profile MSMEsamsarmaÎncă nu există evaluări
- Hospital Waste Management An Insight Approach: NtroductionDocument47 paginiHospital Waste Management An Insight Approach: NtroductionAvijit Mitra MustafiÎncă nu există evaluări
- Amended Nellore DPDocument19 paginiAmended Nellore DPsuryanathÎncă nu există evaluări
- Washer & Dryer SpecsDocument3 paginiWasher & Dryer SpecssamsarmaÎncă nu există evaluări
- Herbal Pest Repellent Potpourri SanitisedDocument1 paginăHerbal Pest Repellent Potpourri SanitisedsamsarmaÎncă nu există evaluări
- Astrology Maha NibandamDocument1 paginăAstrology Maha NibandamNihal SenÎncă nu există evaluări
- SASBE Call For PapersDocument1 paginăSASBE Call For Papersanup8800% (1)
- L&T Limited: About The CompanyDocument2 paginiL&T Limited: About The CompanySai SanjeevareddyÎncă nu există evaluări
- Wise SpendingDocument5 paginiWise SpendingFatiyarrÎncă nu există evaluări
- Uncovering CLIL 1 PDFDocument6 paginiUncovering CLIL 1 PDFrbiv0770Încă nu există evaluări
- Asafa Book Oromuma PDFDocument183 paginiAsafa Book Oromuma PDFgemechuÎncă nu există evaluări
- Wonderlic Scholastic Level Exam Sample Questions: AnswersDocument1 paginăWonderlic Scholastic Level Exam Sample Questions: AnswersElize FontesÎncă nu există evaluări
- BSC6900 RNC Step CommissionDocument6 paginiBSC6900 RNC Step CommissionFrancisco Salvador MondlaneÎncă nu există evaluări
- Swot Analysisdoc MartensDocument2 paginiSwot Analysisdoc MartensaswertyÎncă nu există evaluări
- Beekeeping Practices Challenge and Honey MarketingDocument24 paginiBeekeeping Practices Challenge and Honey MarketingBrook Legese Dadhe 23926007Încă nu există evaluări
- Test A NN4 2020-2021Document2 paginiTest A NN4 2020-2021Toska GilliesÎncă nu există evaluări
- Habits of Mind HandoutDocument2 paginiHabits of Mind Handoutapi-240193026Încă nu există evaluări
- Landon AlexanderDocument6 paginiLandon Alexanderapi-455881201Încă nu există evaluări
- 2015 Nutrition Month Celebration Narrative ReportDocument2 pagini2015 Nutrition Month Celebration Narrative ReportBenjie Modelo ManilaÎncă nu există evaluări
- Reconfigurable Diffractive Antenna Based On Switchable Electrically Induced TransparencyDocument12 paginiReconfigurable Diffractive Antenna Based On Switchable Electrically Induced TransparencyAnuj SharmaÎncă nu există evaluări
- Accomplishment Teachers BoothDocument3 paginiAccomplishment Teachers Boothjosephine paulinoÎncă nu există evaluări
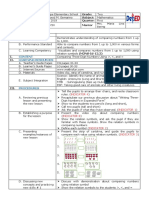
- Comparing Numbers (2021 - 06 - 19 01 - 35 - 12 UTC) (2021 - 08 - 06 04 - 51 - 25 UTC)Document3 paginiComparing Numbers (2021 - 06 - 19 01 - 35 - 12 UTC) (2021 - 08 - 06 04 - 51 - 25 UTC)ALLinOne BlogÎncă nu există evaluări
- SCOPUS Guide For Journal Editors ELSEVIERDocument75 paginiSCOPUS Guide For Journal Editors ELSEVIERKhis HudhaÎncă nu există evaluări
- Digital Logic and Computer Organization: Unit-I Page NoDocument4 paginiDigital Logic and Computer Organization: Unit-I Page NoJit AggÎncă nu există evaluări
- Higher EducationDocument19 paginiHigher EducationAnonymous pxy22mwps5Încă nu există evaluări
- 1machine Learning With PythonDocument12 pagini1machine Learning With PythonAmbika ThakurÎncă nu există evaluări
- 260 Day SWHW Bible Reading PlanDocument12 pagini260 Day SWHW Bible Reading PlanWildoleanderÎncă nu există evaluări
- IPCR Portfolio MOVs TrackerDocument10 paginiIPCR Portfolio MOVs TrackerKris Tel Delapeña ParasÎncă nu există evaluări
- Introduction To Deep Learning: Le Hoang Nam Namlh@hanu - Edu.vnDocument33 paginiIntroduction To Deep Learning: Le Hoang Nam Namlh@hanu - Edu.vnKhoa Tran NgocÎncă nu există evaluări
- Social Psychology ReflectionDocument3 paginiSocial Psychology Reflectionapi-325740487Încă nu există evaluări
- Ade 149Document74 paginiAde 149matt_langioneÎncă nu există evaluări